DIEP Flap Breast Reconstruction
Pierre M. Chevray
DEFINITION
Breast reconstruction following mastectomy can be accomplished with prosthetic breast implants, autologous tissue flaps, or a combination of the two.
Autologous tissue flaps from the lower abdomen are capable of creating the most natural, lasting, and maintenancefree reconstructed breasts with the highest long-term patient satisfaction when compared to other methods of breast reconstruction.1
Autologous tissue flaps have donor-site morbidity and require longer and more complex surgery, with a longer recovery period, compared to implant-based breast reconstruction.
Techniques to harvest lower abdominal flaps of skin and subcutaneous tissue for breast reconstruction have evolved from the pedicled TRAM flap, to the free TRAM flap, to the muscle-sparing free TRAM flap, to the DIEP flap, to the SIEA flap, in order to minimize donor-site morbidity.2
The DIEP (Deep Inferior Epigastric Perforator) flap has become the most popular lower abdominal free flap used for breast reconstruction because of its balance of sparing rectus abdominis muscle function while still providing a well-vascularized and reliable flap of skin and subcutaneous tissue.3,4,5
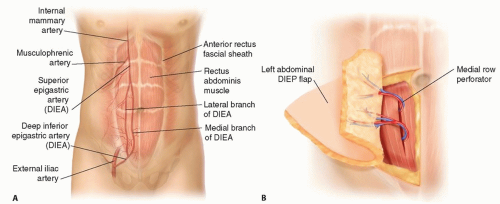 FIG 1 • A. Deep inferior epigastric artery (DIEP) flap anatomy showing a right hemiabdominal DIEP flap skin paddle overlying the right rectus abdominis muscle containing the medial and lateral branches of the deep inferior epigastric (DIE) artery, which gives off the medial and lateral row of perforators. B. The left hemiabdominal DIEP flap is reflected laterally, as it would be during exposure of the medial row of perforators. |
ANATOMY
The vascular pedicle of the DIEP flap is the deep inferior epigastric (DIE) artery and veins, and their branches which perforate through the rectus abdominis muscle (perforators), into the subcutaneous fat of the anterior abdominal wall.
The DIE vessels originate from the external iliac vessels in the pelvis, course anteriorly and superiorly, in the retroperitoneal plane, to the inferolateral border of the rectus abdominis muscle. The DIE vessels continue superiorly, within the rectus sheath, on the deep surface of the rectus abdominis muscle, from which branches to the muscle and perforators into the overlying flap tissue originate. Terminal branches of the DIE vessels coalesce with the terminal branches of the deep superior epigastric vessels (FIG 1).
The single most common branching pattern of the DIE artery is that it bifurcates into two parallel branches that course superiorly on the underside of the rectus abdominis muscle. One branch runs along the medial side of the muscle, giving rise to the “medial row” of perforators, and the other runs along the lateral side of the muscle, giving rise to the “lateral row” of perforators. However, this branching pattern is variable.
Generally, lateral row perforators pierce the muscle perpendicular to the plane of the flat, straplike, rectus abdominis muscle and are easier to dissect compared to medial row perforators, which tend to travel obliquely, from medial
to lateral, and superior to inferior, through the muscle and require dissection along greater distances within the muscle when compared to lateral row perforators.
The limits of the DIEP flap skin paddle are several centimeters superior to the superior edge of the umbilicus, inferiorly to the level of the pubic bone, and laterally to the anterior axillary line. It is possible, usually in younger and thinner patients, to transfer this entire lower abdominal flap based on the perforators from one DIE vascular pedicle.
The skin paddle of lower abdominal flaps has been divided into zones.6 Zone 1 is the paramedian region of the flap skin paddle overlying the rectus abdominis muscle and is the best perfused area of the flap. Zone 2 is lateral to Zone 1. Zone 3 is the mirror image of Zone 1, on the opposite side of the vertical midline. Zone 4, lateral to Zone 3, is the furthest from the perforators and thus the least well-perfused zone and most likely to suffer fat necrosis.
Selecting which perforators to keep, and which are not necessary and can be sacrificed, is one of the critical decisions during this operation and requires the most experience and judgment.
Generally, the single largest perforator will perfuse Zone 1 of a DIEP flap. However, in most breast reconstructions, Zones 1 and 2 are necessary to reconstruct a large enough breast.
Zones 1, 2, and 3, and sometimes Zone 4, can be perfused by including more perforators.
The rectus abdominis muscle is segmentally innervated, and the skin paddle of the DIEP flap receives sensory innervation from the thoracoabdominal branches of the intercostal nerves T7-T11, which run between the internal oblique and transversus abdominis muscles and then enter the lateral border of the anterior rectus sheath.
These thoracoabdominal nerves run roughly transversely, just deep, and within the rectus abdominis muscle along with the accompanying vascular branches of the intercostal arteries and veins to anastomose with the DIE vessels, which run roughly vertically.
The sensory nerve fibers run with the perforators through the rectus abdominis muscle and anterior rectus sheath, into the overlying subcutaneous tissue of the DIEP flap, to innervate the skin. The motor fibers branch into the substance of the rectus abdominis muscle to innervate it.
These motor and sensory nerves run superficial to the DIE vessels, and for all practical purposes, must be divided to harvest and transfer the DIEP flap. Some surgeons repair the nerves that are divided.
PATHOGENESIS
The DIEP flap is most commonly used for breast reconstruction following mastectomy for treatment of breast cancer, or risk reduction in patients with a genetic increased risk of breast cancer such as BRCA 1 or 2 gene mutations.
NATURAL HISTORY
PATIENT HISTORY AND PHYSICAL FINDINGS
The DIEP flap can be used for total, or partial, breast reconstruction in patients who have had a mastectomy or partial mastectomy (lumpectomy, segmental mastectomy), respectively.
IMAGING
CT and MR angiography is used by some surgeons to visualize the DIE vascular pedicle and perforators preoperatively. Some believe this can decrease operative times; however, the author does not use preoperative imaging of any kind.
NONOPERATIVE MANAGEMENT
Breast reconstruction has been shown to improve the quality of life of patients who have had a mastectomy.
The Women’s Health and Cancer Rights Act of 1998, a federal law in the United States, mandates commercial health insurance companies to cover breast reconstruction after a mastectomy, surgery on the opposite breast to improve breast symmetry, and breast prostheses. Despite this law, less than half of patients who have a mastectomy in the United States have breast reconstruction.
Nonsurgical treatment would include using an external breast prosthesis, which fits into a brassiere cup or is part of a custom-made brassiere.
SURGICAL MANAGEMENT
Preoperative Planning
The objective of the operation is to improve the quality of life of the mastectomy patient by reconstructing a breast mound that is as similar to a natural breast as possible.
Absolute contraindications for this operation are prior full abdominoplasty or uncorrectable hypercoagulable state.
Relative contraindications are a body mass index greater than 40 kg/m2, hypercoagulable state, previous abdominal liposuction, and prior abdominal surgery that may compromise the flap or abdominal wall.
The risks of the surgery to be discussed with the patient include the risks of surgery in general (infection, bleeding, pain, scarring, hematoma, seroma, and delayed healing) and the specific risks of this surgery, which are abdominal hernia, bulge, weakness, and partial or total flap loss.
For immediate breast reconstruction, the incisions for the mastectomy are discussed with the breast surgeon. A common issue is, should a patient with ptotic breasts who would like smaller or more lifted reconstructed breasts have a nipple-sparing mastectomy (NSM), even if it is oncologically acceptable? If yes, how long after the NSM and DIEP flap reconstruction will you perform a mastopexy that involves a periareolar incision?
Anecdotally, the author likes to wait at least 6 months.
Alternatively, the patient may be treated with a lumpectomy and oncoplastic mastopexy and complete any adjuvant treatments and then undergo NSM and DIEP flap breast reconstruction.
A third option, in patients without breast cancer such as patients with BRCA mutations, is to have a mastopexy or breast reduction first and then, 6 or more months later, undergo NSM and DIEP flap reconstruction.
Preoperative Markings
Preoperatively, with the patient standing upright, mark the anterior midline from the sternal notch down to the pubis. Mark both inframammary folds (IMFs).Then draw a horizontal line from the most inferior point of each IMF across the midline to the opposite IMF to determine if one side is lower or higher than the other side (FIG 2).
Also with the patient standing, mark the superior flap incision line. This is typically about 2 cm superior to the superior border of the umbilicus but can vary from the level of the superior border of the umbilicus, up to about 5 cm above this.
This transverse line curves inferiorly as it is extended laterally in both directions, and generally ends several centimeters lateral and superior to the anterior superior iliac spine (ASIS).
The lower transverse abdominal incision is also marked preoperatively with the patient standing. This is typically drawn in the natural suprapubic crease and extends laterally, curving gently upward to meet the superior incision line several centimeters superior and lateral to the ASIS (see FIGS 2 and 3).
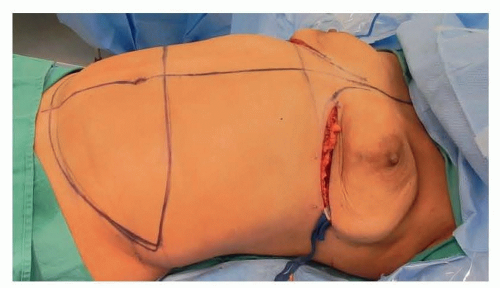 FIG 2 • Patient prepared and draped with arms abducted at 90 degrees on arm boards. The vertical midline, bilateral inframammary folds (IMF), horizontal extension of the nadir of both IMF, and the proposed DIEP flap skin paddles have been marked preoperatively with the patient standing. Bilateral nipple-sparing mastectomies via IMF incisions have been completed. |
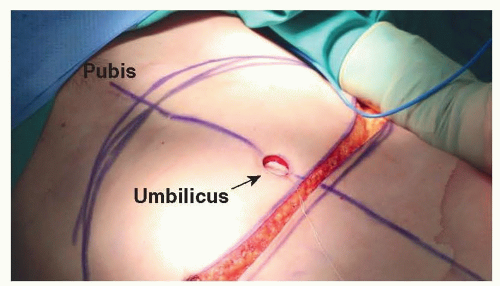 FIG 3 • Initial DIEP flap harvest with patient supine. (Note that in all intraoperative photos, the patient’s head is to the right.) The umbilicus has been cored out from the DIEP flaps, and the upper abdominal incision has been made. The umbilicus has been tagged at its 12 o’clock position with a suture, which will be used later to find the umbilicus and bring it out for insetting once the abdominal donor site has been closed. Note that the initial, more superior, upper and lower abdominal incision markings, which were made preoperatively, have both been lowered by about 2 cm based on an intraoperative pinch/grab evaluation of the abdominal donor site with the patient’s head and back raised to 45 degrees. |
Positioning
The patient is positioned supine with the arms abducted 90 degrees on arm boards. Alternatively, if no axillary lymph node surgery is planned, the arms may be tucked. This allows for easier positioning of a dual head operating microscope for two surgeons, but care must be taken not to injure the patient’s hands and arms when raising the patient’s head and back to close the abdominal donor site.
The operating table may be reversed (turned 180 degrees) underneath the patient, in what is sometimes called a “C-arm position.” This allows the head and back to be raised nearly to 90 degrees upright, which some surgeons desire for evaluating insetting and shaping of the DIEP flap.
TECHNIQUES
In immediate breast reconstruction, DIEP flap harvest can begin at the abdomen at the same time the breast surgeon is performing the mastectomy at the chest. Alternatively, the DIEP flap surgery can begin after the breast surgeon is finished.
Typically, the patient cannot be paralyzed until the breast surgeon has completed any axillary lymph node surgery, and this may make dissection of perforators at the abdomen difficult due to the contraction of the rectus abdominis muscle when stimulating the motor nerves with the electrocautery.
In a unilateral breast reconstruction, assess if a hemi-DIEP flap will provide sufficient volume and skin surface for the reconstruction or if tissue across the midline needs to be harvested.
Once the patient is under general anesthesia, raise the head and back of the patient to about 45 degrees, or more, and perform a pinch/grab test to assess if the abdominal donor site can be closed after flap harvest along the marked incision lines. Raise or lower the upper abdominal incision line to adjust.
The upper abdominal incision is commonly at the level of the superior border of the umbilicus or up to several centimeters superior to this. Return the patient to the supine position. FIG 3 shows an example where the initially marked upper and lower abdominal incision lines were both lowered intraoperatively by about 2 cm after the pinch/grab test of the donor site.
▪ DIEP Flap Harvest
Incision and Flap Elevation
The abdominal incisions are made. The superior incision is beveled superiorly to capture more subcutaneous tissue volume with the flap and to decrease the thickness of the cut edge of the upper abdominal donor-site flap. This creates a better thickness match between the upper and lower cut edges of the abdominal donor-site incision at closure.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree