Figure 20.1
(a) Epidermal sloughing on face with affection of the eyes and lips. (b) Epidermal sloughing on the back. (c, d) Hemorrhagic flaccid blisters on upper and lower limbs
The condition was preceded by high grade fever 5 days earlier along with upper respiratory tract infection and epigastric pain for which she was prescribed co-trimoxazole (Septrin®), diclofenac sodium (Voltaren®), ranitidine tablets (Zantac®) for 4 days. She noticed no improvement and consulted another doctor, who shifted her to azithromycin tablets (Zithromax®) and ibuprofen tablets (Brufen®). The following day the patient developed the present condition.
1.
What is your diagnosis?
(a)
DRESS
(b)
Stevens Johnson syndrome
(c)
Toxic epidermal necrolysis
(d)
Erythroderma
(e)
Acute generalized exanthematous pustulosis
2.
The drug associated with confirmed high risk of this skin disease is:
(a)
Ibuprofen
(b)
Co-trimoxazole
(c)
Diclofenac sodium
(d)
Azithromycin
(e)
Ranitidine
The patient was hospitalized in the intensive care unit where blood pressure was 110/70, pulse 90 /min with normal rhythm and temperature was 39 °C. CBC was normal, ESR is high (100 mm/min), elevated SGOT, SGPT (less than triple the normal values), low level of potassium (2.8 mmol/L), elevated level of urea and creatinine (113 mg/dL, 2.3 mg/dL) and normal glucose (post prandial: 135 mg/dL) and bicarbonate levels (22 mEq/L). All medications were stopped. Supportive treatment was given, fluid and electrolytes were corrected. Urea and creatinine became normal in 24 h. Then, Cyclosporine 5 mg/kg was started in addition to plasmapheresis which was done every other day for 2 weeks. Three weeks later, there were significant healing of eroded skin all over the body while oral lesions showed little improvement and symblepharon developed in the eyes (Fig. 20.2).
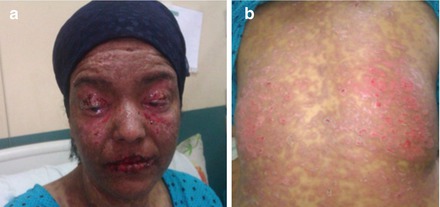
Figure 20.2
Improvement of skin lesions after 3 weeks
Diagnosis: Toxic epidermal necrolysis (Lyell’s disease).
Answers
1.
(c)
2.
(b)
Discussion
Toxic epidermal necrolysis (TEN) is a life threatening adverse drug reaction (mortality rate 30 %) involving widespread keratinocyte apoptosis. TEN is characterized by widespread sloughing of the skin and the mucosa. Drug-induced CD8 cell activation is highly specific for particular HLA allotypes, placing certain populations at a greater risk for developing TEN [1].
The majority of cases of toxic epidermal necrosis are the result of a hypersensitivity reaction to a drug. Other causative agents include Mycoplasma pneumonia, dengue virus, cytomegalovirus, and contrast medium [1]. According to the 2008 Euro-SCAR study [2], drugs associated with confirmed high risk of SJS/TEN includes nevirapine, lamotrigine, carbamazepine, phenytoin, phenobarbital, cotrimoxazole, other anti-infective sulphonamides, sulphasalazine, allopurinol, oxicam-non steroidal anti-inflammatory drugs;
TEN most often begin with a prodrome of fever, malaise, anorexia, pharyngitis, headache, and rash, A painful macular exanthem appears in a symmetrical distribution on the face and trunk, spreading to the extremities. The skin develops the Nikolsky sign, whereby gentle lateral pressure causes the epidermis to slide over the basal layer. Blisters evolve and large sheets of epidermis slough off, leaving an exposed, weeping dermis. Ocular involvement with adhesions and ulceration can result in photophobia, pain, and loss of vision. TEN is more commonly seen with HIV, systemic lupus erythematosus collagen vascular diseases and malignancy [3]. Histologically, sections of skin from TEN exhibit widespread keratinocyte apoptosis. There is separation at the dermoepidermal junction and a mild mononuclear infiltrate is seen in the dermis [4].
TEN is considered part of a group of cutaneous hypersensitivity reactions with a spectrum of severity; erythema multiforme, followed by Stevens-Johnson syndrome (SJS) and TEN. SJS involves less than 10 % of the total body surface area, whereas TEN involves more than 30 % of the total body surface area. Total body surface area involvement between 10 and 30 % is known as SJS-TEN overlap [5].
Infection is the most common cause of death in TEN. Other fatal complications include pulmonary embolism, adult respiratory distress syndrome, gastrointestinal hemorrhage, as well as cardiac and renal failure [6].
Distinguishing TEN syndrome from the other major potentially life-threatening cutaneous drug reactions with similar clinical features—Drug reactions with eosinophilia and systemic symptoms (DRESS), acute generalized exanthematous pustulosis (AGEP), and erythroderma (exfoliative dermatitis)—is an important concern because treatment varies among these conditions. Clinically, the onset of eruption of SJS/TEN, AGEP, and erythroderma after drug ingestion is shorter and subsides sooner than in DRESS syndrome.
DRESS syndrome is characterized by facial edema, morbilliform eruption, pustules, exfoliative dermatitis, tense bullae, and possible target lesions. Lymph node enlargement, hepatitis and eosinophilia are also found [7].
Related posts:
 An Elderly Patient with a Generalized Pruritic Eruption
A Healthy African Child with Blisters
An Elderly Patient with a Generalized Pruritic Eruption
A Healthy African Child with Blisters
 A 52 Year Old Man with Cerebriform Vegetating Masses on the Scalp
A 52 Year Old Man with Cerebriform Vegetating Masses on the Scalp
 Single Step Multivariant Analysis of Serum Autoantibodies in Autoimmune Blistering Diseases Using BIOCHIP® Mosaic Technology
Single Step Multivariant Analysis of Serum Autoantibodies in Autoimmune Blistering Diseases Using BIOCHIP® Mosaic Technology
 A Chronically Ill Teenager with Blisters and Scars
A Chronically Ill Teenager with Blisters and Scars
 A Man with a Blistering Rash
A Man with a Blistering Rash
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


