div class=”ChapterContextInformation”>
12. Seborrheic Dermatitis
Keywords
Seborrheic dermatitisDandruffSebaceous glandMalassezia spp.Epidermal barrierTreatmentAntifungalsAnti-inflammatory agentsOral isotretinoinIntroduction
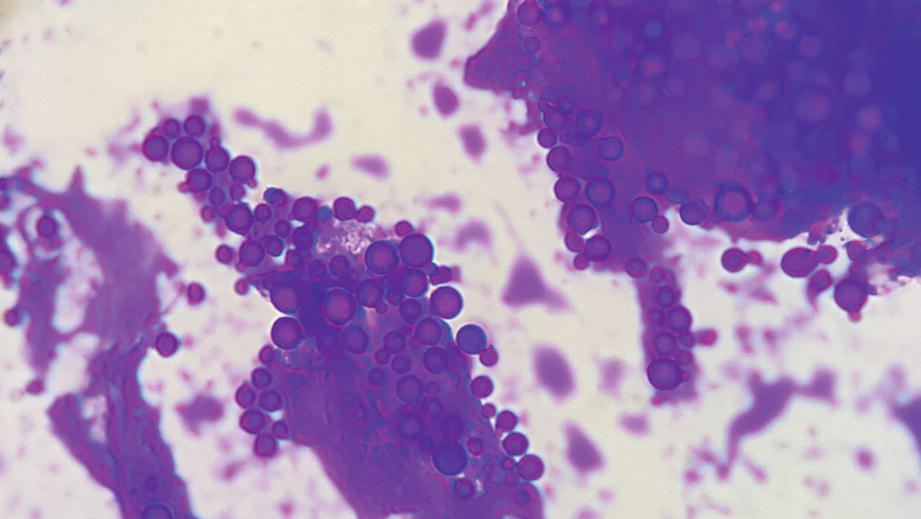
Smear with Gram stain shows abundant yeasts (100×)

Malassezia spp . can be isolated if Dixon’s agar culture is performed
Diagnostic Procedures and Laboratories Required Before Starting Treatment
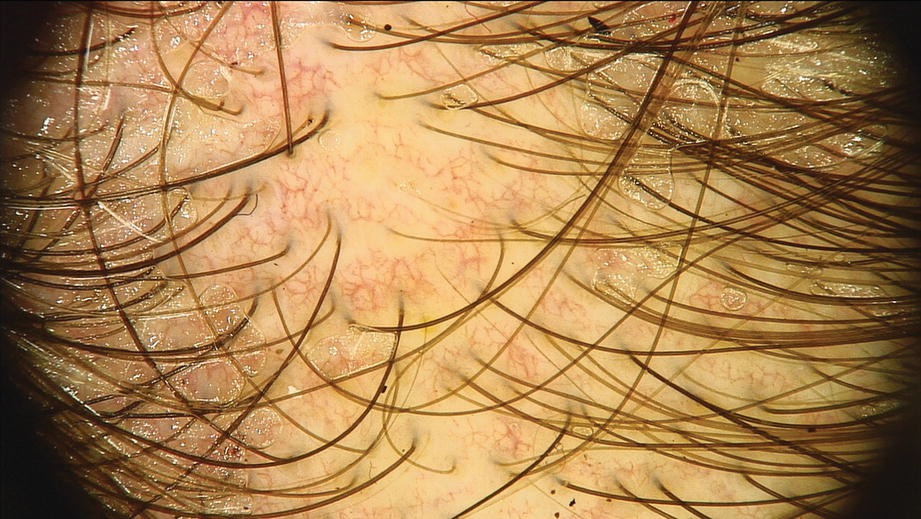
Increased number of arborizing vessels (dermoscopy 70×)

Abundant yellow greasy scales in a severe case (dermoscopy 70×)
Treatment Strategy: A General Introduction
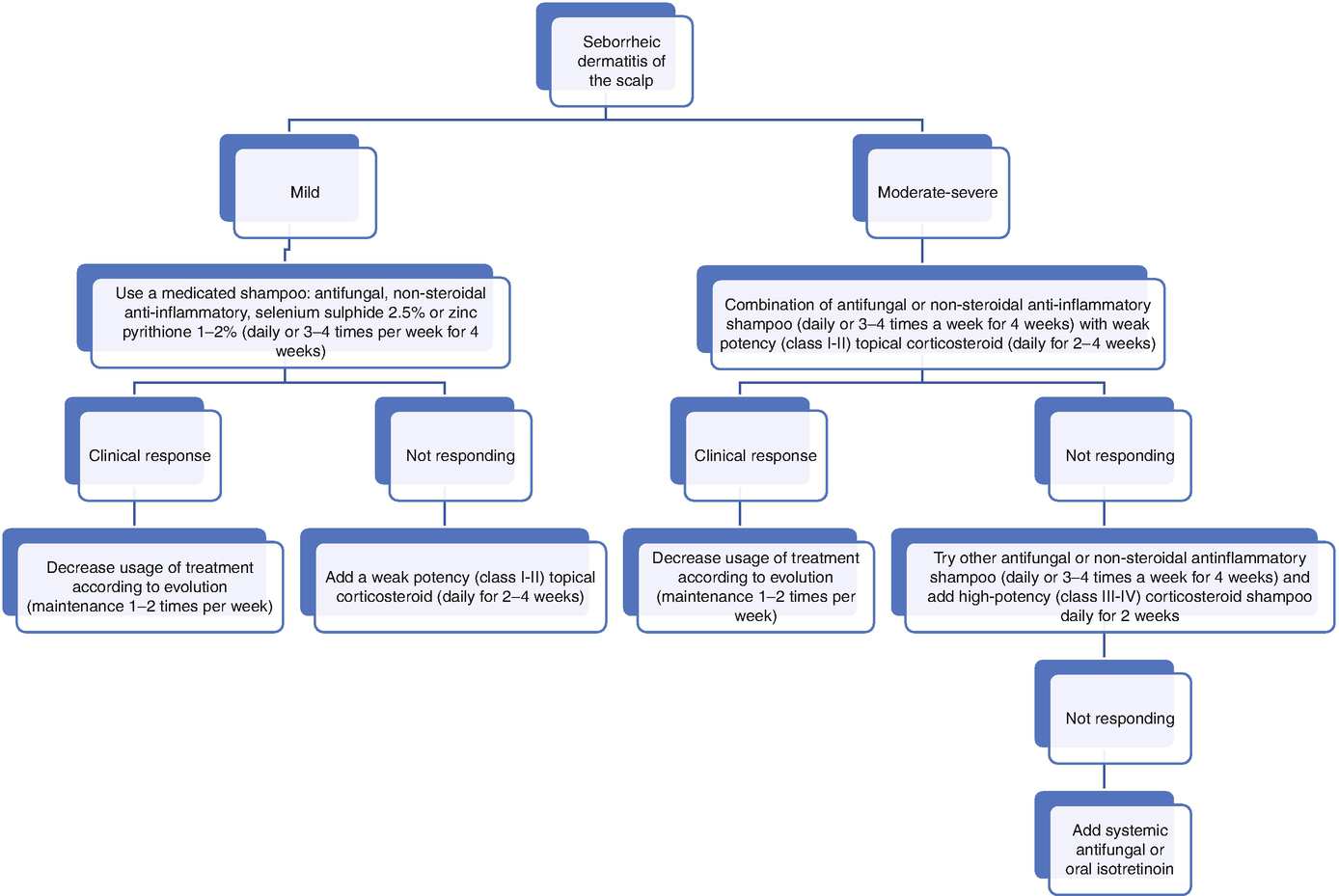
Scalp seborrheic dermatitis treatment options
First-line treatments |
Topical |
A. Antifungals |
B. Anti-inflammatory agents |
a. Corticosteroids |
b. Non-steroidal anti-inflammatory agents |
1. Bisabolol |
2. Glycyrrhetinic acid |
3. Climbazole/piroctone olamine |
4. Promiseb® |
5. Lactoferrin |
Second-line treatments |
Topical |
A. Selenium sulfide |
B. Keratolytic agents |
a. Coal tar |
b. Salicylic acid/lipohydroxy acid |
c. K301 |
C. Phototherapy |
Systemic |
A. Itraconazole |
B. Terbinafine |
C. Fluconazole |
D. Pramiconazole |
E. Isotretinoin |
Third-line treatments |
Topical |
A. Aloe vera |
B. Borage and tea tree oils |
C. Quassia amara |
D. Solanum chrysotrichum |
E. Homeopathic mineral medicine |
F. Vitamins |
First-Line Treatments
Topical Antifungals
Scalp seborrheic dermatitis treatment regimensa
Drug | Formulation | Instructions for use |
|---|---|---|
Topical antifungals | Ciclopirox 1–1.5% Ketoconazole 1–2% Zinc pyrithione 1–2% Shampoo or lotion | Daily or 3–4 times per week for 4 weeks or until clinical remission Maintenance therapy: once or twice per week for several months to prevent relapse |
Non-steroidal anti-inflammatory agents | Piroctone olamine, bisabolol, glycyrrhetic acid, lactoferrin, and Promiseb® Shampoo or lotion | Daily or three to four times per week for 4 weeks or until clinical remission Maintenance therapy: once or twice per week for several months to prevent relapse |
Low-potency topical corticosteroids (classes I–II) | Class I potency Hydrocortisone 1% Class II potency Desonide 0.05% Lotion | Daily for 2–4 weeks and then decrease |
High-potency topical corticosteroids (class III–IV) | Class III potency Fluocinolone acetonide 0.01% Class IV potency Clobetasol propionate 0.05% Shampoo or lotion | Daily for 2 weeks and then decrease |
Second-line treatments | Selenium sulfide 2.5% Shampoo or lotion | Daily or 3–4 times per week for 4 weeks or until clinical remission Maintenance therapy: once or twice per week for several months to prevent relapse |
Keratolytics | Tar 1–2%, salicylic acid 3% Shampoo or lotion | Daily or 3–4 times per week for 4 weeks or until clinical remission Maintenance therapy: once or twice per week for several months to prevent relapse |
Systemic antifungals | Itraconazole 100 mg caps | 200 mg/day for 1 week, then 200 mg/day for 2 days/ per month for 2–3 months |
Terbinafine 250 mg caps | Continuous: 250 mg/day for 4–6 weeks. Intermittent: 250 mg/day for 12 days a month for 3 months | |
Fluconazole 150 mg caps | 50–300 mg weekly for 2–4 weeks | |
Oral isotretinoin | 5–10 mg/day or three times per week for several months |
Topical Anti-inflammatory Agents
Corticosteroids
They are the most effective drugs in clearing SD signs and symptoms (inflammation, erythema, and pruritus). They can be used alone or in combination with antifungal agents; however, their prolonged use is not recommended due to possible side effects (telangiectasias, hypertrichosis, atrophy, and perioral dermatitis). Prescribe a weak-moderate topical corticosteroid (classes I and II) daily for 2–4 weeks. The authors prefer a lotion versus a shampoo to avoid unnecessary exposure of other body areas. Treatment is then gradually discontinued [1, 2, 23–25].
Non-steroidal Anti-inflammatory Agents
These drugs inhibit Malassezia species growth through their anti-inflammatory, antimycotic, keratolytic, and antioxidant effects. They are usually combined with other compounds in shampoos and lotions and are applied daily or 3–4 times per week. These drugs are generally well-tolerated, effective, viable, and safe. Adverse effects may include pricking sensation, stinging, itching, burning, erythema, and viral gastroenteritis [1, 2, 26–28].
Bisabolol
Monocyclic sesquiterpene alcohol with antioxidant and anti-inflammatory properties that downregulates the human polymorphonuclear neutrophils’ release. In SD, it has an anti-inflammatory effect more specific than corticosteroids and anti-fungal drugs but is probably not very potent in monotherapy [1, 2, 28, 29].
Glycyrrhetinic acid
It is an ingredient of the black licorice with anti-microbial and anti-inflammatory properties. It inhibits the 11-β-hydroxysteroid hydroxygenase enzyme in the steroid metabolism, potentiating the anti-inflammatory effects [1, 2, 30].
Climbazole/piroctone olamine
Piroctone olamine is an ethanolamine salt with antifungal properties which creates iron ion complexes in the fungal cell membrane, and climbazole is an imidazole antifungal agent that blocks P-450 [1, 2, 26, 31, 32].
Promiseb®
This combines many active ingredients (e.g., glycyrrhetinic acid and piroctone olamine) to enhance the anti-inflammatory and anti-fungal activity against SD [1, 2, 33].
Second-Line Treatments
Selenium Sulfide
Heavy metal salt with antifungal properties that promote the shedding of the infected stratum corneum. It is indicated in shampoo at 2.5% daily or 3–4 times per week for 4–8 weeks. Adverse effects include pruritus, burning sensation, and hair/scalp discoloration. Other effective alternatives include precipitated sulfur 3% and colloidal sulfur 5% [35, 36].
Keratolytic Agents
Coal Tar
A complex mixture of phenols, polycyclic aromatic hydrocarbons, and heterocyclic compounds with antifungal, anti-inflammatory, anti-itch, and keratolytic properties. Commercial presentations include shampoos and lotions to be applied 2–3 times per week for 4–8 weeks. Side effects include skin irritation, sun sensitivity, allergic reactions, and skin discoloration. Its use in pregnancy and breastfeeding is not recommended [37–40].
Salicylic Acid/Lipohydroxy Acid (LHA)
Its mechanism of action includes exfoliation, stimulation of epidermal renewal, and antimicrobial properties against Malassezia spp. Apply daily or 3–4 times per week for 4–8 weeks for scale removal [41].
K301
Topical solution with a mixture of urea, propylene glycol, and lactic acid with keratolytic, exfoliating, anti-fungal, and hydrating properties. It is applied daily during 4 weeks and then three times per week for another month. Adverse effects included smarting pain, redness, burning, rash, itching, eczema, and ulceration [42].
Phototherapy
UVB therapy is useful in some inflammatory skin conditions by inducing immunosuppression, T cell apoptosis, and reducing cell proliferation. There is not an established phototherapy regimen in DS, but the administration of narrow-band UVB three times per week has proved to be effective until signs disappear completely. Home devices are available for the scalp and can be utilized in association with antifungals and anti-inflammatory treatments [43–46].
Systemic Treatment
Itraconazole
A triazole with high keratinophilic and lipophilic properties and a good safety profile. This drug also has an anti-inflammatory effect inhibiting the 5-hypoxygenase metabolite synthesis. The recommended treatment includes 100 mg twice per day for 1 week followed by pulse administration of 200 mg/day during the first 2 days of the months for 2–3 months. Side effects include nausea, vomiting, diarrhea, headache, stomach discomfort, or dizziness; however, these are rare with pulse treatment [47–51].
Terbinafine
Antimycotic with antioxidant and anti-inflammatory properties against dermatophytes, molds, dimorphic fungi, and other pathogenic yeasts. The recommended dose is 250 mg per day for 4–6 weeks or as intermittent treatment (250 mg/day for 12 days a month for 3 consecutive months). Adverse effects include mild tachycardia, insomnia, gastrointestinal discomfort, migraine, cutaneous rash, hypogeusia, and hyposmia [52–54].
Fluconazole
Broad-spectrum bistriazole derivative that inhibits dermatophytes, yeasts, and dimorphic fungi. It has been demonstrated to be effective in the sebum excretion at a dose of 150 mg or 300 mg per week for 4–8 weeks. Adverse effects include elevated liver function tests and nausea [55–57].
Ketoconazole
Not indicated for DS because of hepatotoxicity risk and testosterone metabolic alterations [58].
Pramiconazole
It is a triazole antifungal agent that inhibits ergosterol synthesis and which has broad activity against Candida sp., dermatophytes, and Malassezia sp. This drug has the best activity against Malassezia spp. due to its high affinity toward cytochrome P450. A single daily dose of 200 mg for 1–4 weeks improves erythema, itching, and desquamation. Adverse events include diarrhea and gastrointestinal discomfort [59–61].
Isotretinoin
Oral isotretinoin decreases the sebum secretion by reducing the sebaceous gland size and stimulating basal sebocyte apoptosis. This drug also has anti-inflammatory properties as it reduces the interleukin production, Toll-like receptor 2 activity, and polymorphonuclear cell migration. Low doses of this drug (5–10 mg/day or three times per week) for several months may be considered as a treatment option for moderate to severe seborrhea. This drug requires effective contraception in women [62–66].
Third- and Fourth-Line Treatments
Aloe vera
Aloe vera has anti-inflammatory, antibacterial, and antifungal properties. This plant has been used widely for the prevention of seborrheic dermatitis and other fungal infections, wound healing, and anesthetic purposes [67, 68].
Borage and Tea Tree Oil (Topical Essential Oils)
Borage oil contains approximately 25% of gamma-linolenic acid (GLA) which is one of the several essential amino acids involved in skin barrier restoration. Tea tree oil (TTO) is obtained from Melaleuca alternifolia leaves and has antimicrobial, anti-inflammatory, antifungal, antioxidant, and anti-skin cancer properties. Terpinen-4-ol is the tea tree oil’s major component which reduces the production of tumor necrosis factor, interleukin-1 (IL-1), IL-8, IL-10, and prostaglandin E2. Tea tree oil is a possible allergen, and contact dermatitis is a possible side effect [69–73].
Quassia amara
It is a small tree from South America with high levels of active phytochemicals (triterpenoid quassinoids) and antimicrobial, anti-inflammatory, and antifungal properties [74].
Solanum chrysotrichum
The main component of this plant (steroidal saponins) has demonstrated antifungal properties against yeast and dermatophytes [75, 76].
Homeopathic Mineral Medicine
Low doses of oral homeopathic medication (potassium bromide, sodium bromide, nickel sulfate, and sodium chloride) are an alternative therapy for SD. Adverse effects are minimal and include stomach discomfort, stomach pain, and nausea [77].
Vitamins
Some nutrients such as essential fatty acids, vitamins A, E, and D, vitamins B1, B2, and B6, niacin, biotin, vitamin C, selenium, zinc, and iron may play a role in the treatment of SD. Biotin (vitamin H) is essential for the long-chain fatty acid synthesis; nicotinamide regulates the cellular inflammation and zinc the sebum production (epithelial differentiation with anti-inflammatory, antibacterial, and antiandrogen properties) . Biotin’s recommended dose is 5–10 mg/day. Patients should be informed to discontinue the drug a few days before laboratory exams as its intake can interfere with lab results [78–84].
Treatment Selection
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


