Dermal Suspension and Parenchymal Reshaping Mastopexy after Massive Weight Loss: Statistical Analysis with Concomitant Procedures from a Prospective Registry
J. Peter Rubin, M.D.
Jeffrey A. Gusenoff, M.D.
Devin Coon, B.A.
Pittsburgh, Pa.
From the Division of Plastic and Reconstructive Surgery, University of Pittsburgh Medical Center, Life after Weight Loss Center.
Received for publication June 28, 2008; accepted September 19, 2008.
Copyright © 2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31819ba1a8
Disclosure: None of the authors has a financial interest to declare in relation to the content of this article.
Background: An increasing number of women are presenting for mastopexy after massive weight loss. The authors analyzed data from a prospective registry of massive weight loss patients who underwent the dermal suspension and parenchymal reshaping mastopexy alone or with concomitant operations to assess safety and efficacy.
Methods: One hundred eight female massive weight loss patients underwent mastopexy. Variables included operative time; time since gastric bypass; body mass index; revision; and complications such as seroma, dehiscence, hematoma, and infection. Univariate analyses were performed to assess outcome measures.
Results: Ninety-one patients underwent mastopexy without implant [mean age, 43.7 ± 9 years; mean intraoperative time, 8.5 ± 3 hours (mastopexy plus concomitant procedures), mean body mass index, 28.3 ± 3.9; mean time since gastric bypass, 27.5 ± 13.4 months; mean follow-up, 7.3 months], whereas 17 had augmentation/mastopexy. Eighty-five of 91 patients (93.4 percent) had multiple procedures performed. Wound dehiscence was the most common complication in 26 patients (29.2 percent); however, breast-specific complications overall occurred in only eight patients (8.8 percent). Body mass index and operative time did not predict an increase in complication rates. Patients who underwent augmentation/mastopexy had a lower current body mass index than those who had mastopexy alone (p = 0.01).
Conclusions: Dermal suspension, parenchymal reshaping mastopexy is a safe, effective, and durable method of treating the deflated breast after massive weight loss. Although patients with massive weight loss are likely to present for longer procedures and have a higher rate of wound-healing complications, these complications occur most frequently in areas other than the breast. (Plast. Reconstr. Surg. 123: 782, 2009.)
As bariatric procedures such as gastric bypass and laparoscopic banding increase in popularity for the surgical treatment of obesity and diabetes, a growing number of women are presenting for breast reshaping after massive weight loss.1,2 The number of mastopexy operations has increased by 12 percent from 2005 to 2006 and by 96 percent since 2000.3 Several procedures have been described to treat the deflated breast after massive weight loss.4–10
Breast deformities after massive weight loss vary significantly. Patients typically present with breast ptosis, medialization of the nipple-areola complex, and extension to a lateral chest roll. Procedures to correct the deflated breast often address the entire aesthetic unit, including the upper abdomen and lateral chest rolls. Augmentation/mastopexy
is another technique used to treat this patient population but can be undesirable because of skin laxity. The goals for mastopexy after massive weight loss include obtaining a youthful, well-contoured breast with upper pole fullness, proper nipple positioning, and a result that maintains its aesthetics over time.
is another technique used to treat this patient population but can be undesirable because of skin laxity. The goals for mastopexy after massive weight loss include obtaining a youthful, well-contoured breast with upper pole fullness, proper nipple positioning, and a result that maintains its aesthetics over time.
Although many techniques exist, there is little information about the safety of this procedure when combined with other procedures, such as abdominoplasty, lower body lift, and brachioplasty. We present a statistical analysis of a large prospective database for the dermal suspension, parenchymal reshaping mastopexy with concomitant operations in the massive weight loss population.
Patients and Methods
The patients included in this study are massive weight loss patients from gastric bypass, laparoscopic banding, or exercise-induced weight loss, and were enrolled in a prospective registry as approved by the Institutional Review Board of the University of Pittsburgh over a 6-year period, with a maximum follow-up of approximately 3 years. An analysis of mastopexy and augmentation/mastopexy patients was performed, examining age, gender, pre–weight loss body mass index (in kilograms per square meter), current body mass index, change in body mass index, operative time, concomitant procedures, and need for revision. Complications included seroma, hematoma, wound dehiscence, cellulitis, abscess, and skin flap necrosis.
All patients enrolled presented with grade II or III ptosis with volume loss and laxity extending to the lateral chest. Severity of breast deformity after massive weight loss ranged from grade 0 to 3, according to the Pittsburgh Rating Scale.11 On the scale, 0 represents a normal breast, 1 represents grade I or II ptosis, 2 represents grade III ptosis,12 and 3 represents a severely deflated breast and/or prominent lateral roll. Patients desiring an increase in volume underwent augmentation mastopexy with a traditional periareolar mastopexy or vertical mastopexy with scar extension in the inframammary fold as necessary. Patients with enough autologous tissue for reconstruction underwent the dermal suspension, parenchymal reshaping mastopexy with selective autoaugmentation, as reported previously by the senior author (J.P.R.).4,5,13,14 All patients received sequential compression devices before, during, and after surgery until the time of discharge. Within the past year, we have added postoperative chemoprophylaxis with enoxaparin (starting 6 hours postoperatively) on all body contouring patients.
Technique
The breasts are marked with a modified Wise pattern, extending laterally to encompass any significant lateral rolls and allow for selective autoaugmentation. After deepithelialization, a parenchymal flap is raised 1 to 1.5 cm thick and elevated to the level of the clavicle bilaterally to allow for dermal suspension. Lateral and medial dermoglandular flaps are raised, supplied by intercostal artery perforators. The central pedicle is secured to the second rib periosteum (the third rib can be used selectively) with braided permanent suture, followed by securing the lateral extension to the third rib periosteum. The medial flap is secured to the third or fourth rib periosteum (Fig. 1). The lateral dermal edge of the lateral parenchymal flap is secured to the chest wall fascia to accentuate the lateral curvature of the breast.
Once the dermal suspension is complete, parenchymal reshaping commences using interrupted and running absorbable sutures to shape the parenchyma laterally, inferiorly, and medially, forcing projection centrally (Fig. 2). Periodic redraping of the skin flaps allows the aesthetic contour to be assessed. The nipple-areola complex often requires scoring of the dermis surrounding it to allow the nipple to assume the correct position in the keyhole pattern. The skin is closed in two layers over a suction drain and a compressive dressing is placed until the first postoperative visit. Drains are usually removed at the first postoperative visit. Representative cases with 1- to 2-year follow-up are shown in Figures 3 and 4.
Statistical Analysis
Statistical computations were performed using Stata SE Version 10.0 (StataCorp., College Station, Texas). Univariate logistic regression analyses were used to examine the influence of the independent variables (i.e., age, body mass index, surgical time, and time since gastric bypass) on the complications of mastopexy with or without concomitant body contouring procedures after massive weight loss. Unpaired t tests were used to determine differences in patient characteristics between mastopexy patients and those who had augmentation/mastopexy. All statistical tests were two-sided, and significance was set to the level of p < 0.05.
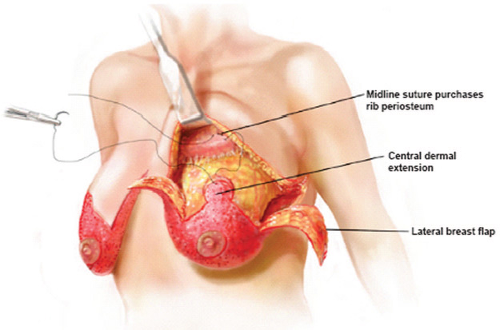 Fig. 1. Drawing demonstrating dermal suspension. After deepithelialization, skin flaps are raised 1 to 1.5 cm thick and undermined superiorly to the level of the clavicle. The central dermoglandular pedicle is secured to the second rib periosteum with permanent braided suture. The third rib can be used selectively. Lateral and medial flaps are raised and secured to rib periosteum at lower levels. (Reprinted with permission from Rubin JP. Mastopexy in the massive weight loss patient: Dermal suspension and total parenchymal reshaping. Aesthetic Surg J. 2006;26:214–222.) |
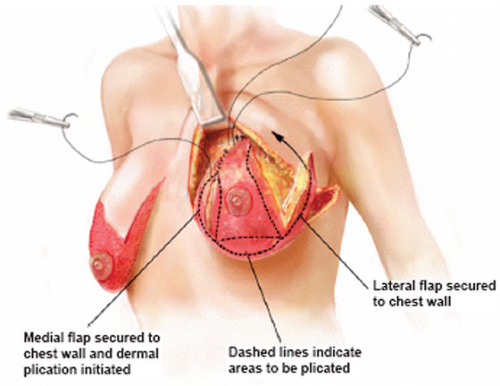 Fig. 2. Drawing demonstrating parenchymal reshaping. After securing the medial and lateral flaps to the chest wall, parenchymal reshaping is performed with interrupted and running absorbable suture to imbricate breast tissue and force projection centrally. (Reprinted with permission from Rubin JP. Mastopexy in the massive weight loss patient: Dermal suspension and total parenchymal reshaping. Aesthetic Surg J. 2006;26:214–222.)
Related posts: One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients One-Stage Mastopexy with Breast Augmentation: A Review of 321 Patients
 Breast Deformities and Mastopexy Breast Deformities and Mastopexy
 Prospective Comparative Clinical Evaluation of 784 Consecutive Cases of Breast Augmentation and Vertical Mammaplasty, Performed Individually and in Combination Prospective Comparative Clinical Evaluation of 784 Consecutive Cases of Breast Augmentation and Vertical Mammaplasty, Performed Individually and in Combination
 Mastopexy Mastopexy
 Facial Skeletal Augmentation with Implants Facial Skeletal Augmentation with Implants
 Rhinoplasty in the Asian Nose Rhinoplasty in the Asian Nose
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|