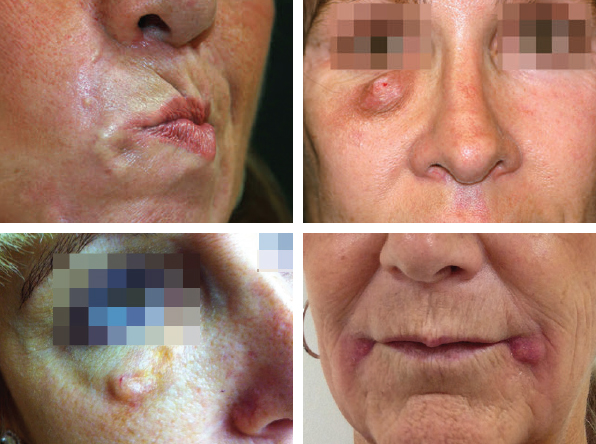
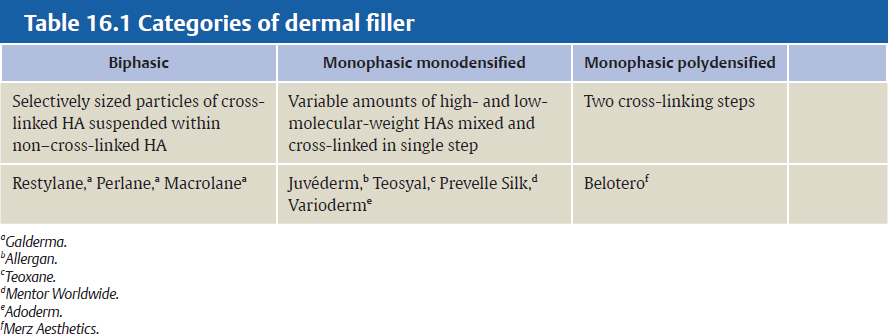
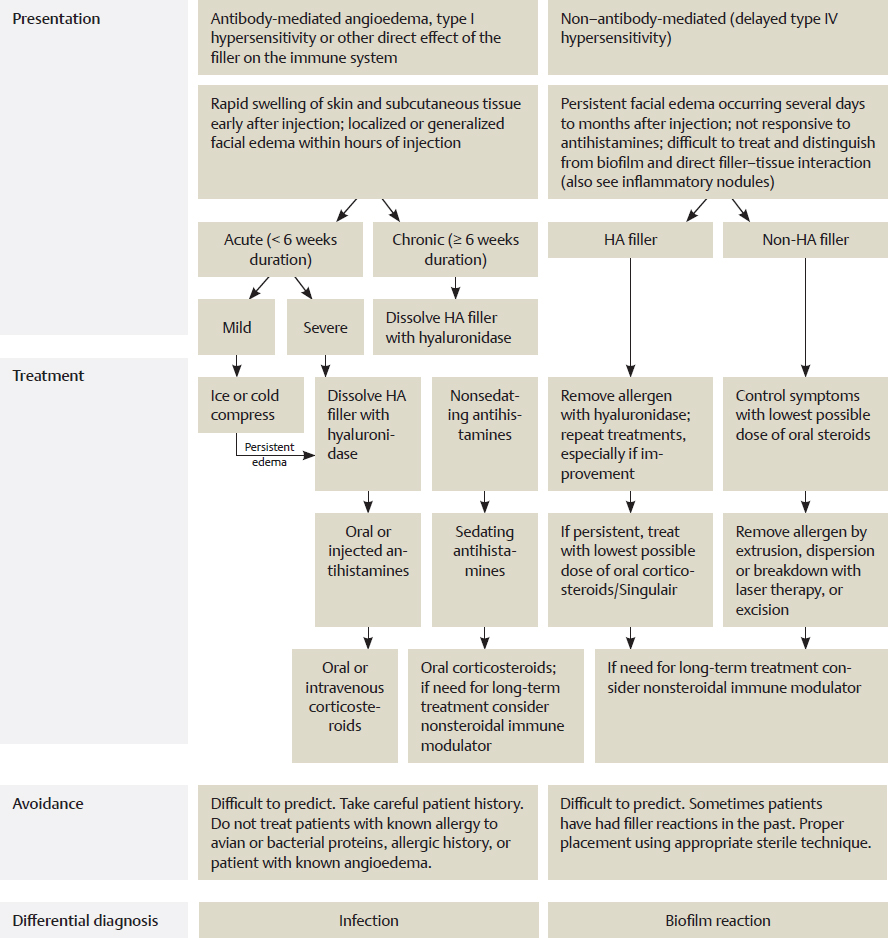
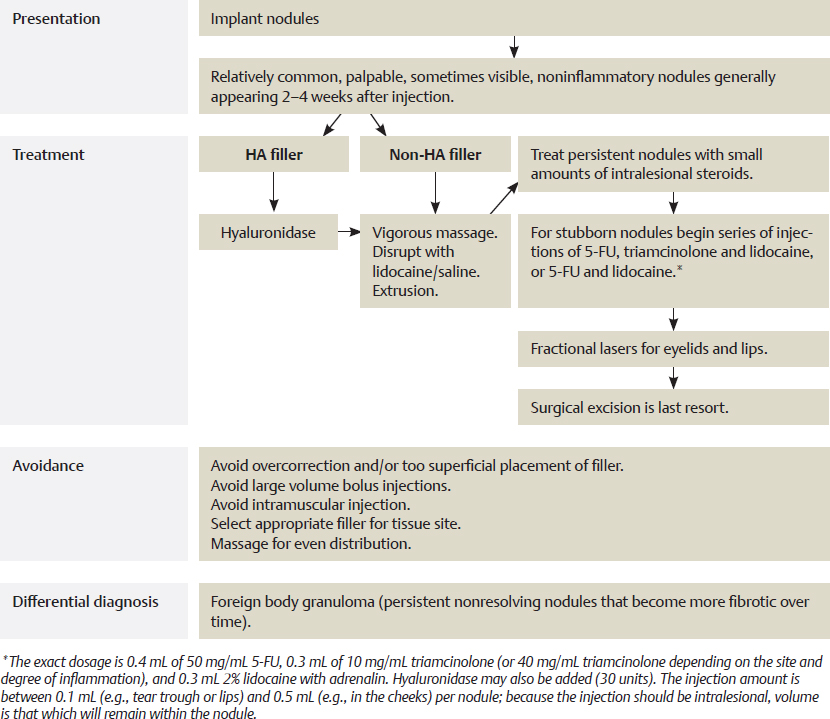
CHAPTER Public awareness and demand for injectable dermal fillers and botulinum neurotoxin treatments continue to grow as more people opt for noninvasive aesthetic rejuvenation and enhancement. This trend is illustrated by recent data from the American Society of Aesthetic Plastic Surgery (ASAPS), which show that dermal filler and neurotoxin treatments have increased by 35 and 39%, respectively, in the past 5 years.1 Along with neurotoxin injections, dermal fillers are the mainstay of most medical aesthetic practices. Recently, the FDA also approved deoxycholic acid, a noninvasive method for removing submental fat, which now joins intense pulse light (IPL) therapy, laser, ultrasonic, and radiofrequency devices to further expand the aesthetic provider’s growing armamentarium. When performed by experienced, well-trained practitioners, adverse events occur in less than 1% of patients, and most of these are minor and short lived.2 However, as treatment indications expand and the number of treatments performed increases, so to do the number and spectrum of adverse events. Although most adverse reactions are mild and transient, more serious complications do occur, leaving patients with long-lasting or permanent functional and aesthetic deficits. It is essential that a practitioner be aware of the spectrum of complications that can occur and be able to recognize, diagnose, and treat these adverse events. Any provider performing injectable treatments should have a comprehensive understanding of the injectate characteristics and capabilities, available injection techniques, and the injection site anatomy, because these are the triad that reduce the risk of an adverse event. This requires expert familiarity with the properties and potential complications of a variety of products, including those that are not available in the injector’s country of practice, because patients may present with adverse reactions to fillers injected abroad. I have had the privilege to serve as a medical director for Merz USA and as a medical advisor to Allergan Corporation assisting practitioners with adverse events and their man agement. I have extensive personal injection experience and have taught anatomy, technique, and adverse event treatment avoidance for over a decade. To prepare this chapter, I reviewed reports in the literature regarding complications with dermal fillers, botulinum neurotoxin, and deoxycholic acid injection and combined this data with my wide-ranging experience to develop recommendations for avoiding and managing complications. Dermal fillers may be classified as biodegradable (moderate and long duration) or nonbiodegradable fillers. Hyaluronic acid (HA) fillers are the most widely used biodegradable fillers in both Europe and the United States and generally have effects lasting 6 to 24 months. HAs are linear polymeric dimers of N-acetylglucosamine and glucuronic acid, which differ in the proprietary methods used to cross-link their dimers, their degree of chain cross-linking, the uniformity and size of their particles, and their concentration. These characteristics all have a significant impact on the clinical effect of these products. Increased cross-linking, concentration, and particle size increase the viscosity and elasticity and the time necessary for degradation by native hyaluronidase. The hydrophilic nature of HA means that the more concentrated and/or large-particle products will tend to absorb more water and thus cause more tissue swelling after injection. HA fillers may be biphasic or monophasic (Table 16.1). Each type of HA has a predictable histologic behavior in the skin affecting its suitability for different indications.3 The different HAs have varying degrees of hardness (G′), which also influence their suitability for a particular procedure. In general, the greater the G′ of the product, the deeper it should be injected. It should be noted that although more concentrated products with a greater degree of cross-linking have a longer duration of effect, they also increase reactivity in the body and thus the risk of inflammation and granuloma formation. Fillers with biodegradable particles that stimulate the body to produce its own collagen have a longer duration of effect and include calcium hydroxylapatite (CaHA; Radiesse [Merz Aesthetics]) and poly-L-lactic acid (PLLA; Sculptra [Galderma]). Radiesse consists of synthetic CaHA microspheres (25 to 40 microns) suspended in a carrier gel. Injection provides immediate correction with long-term deposition of new collagen surrounding the microspheres, which contributes to an average duration of effect of 15 months.4 PLLA is a synthetic polymer that provides soft tissue augmentation through stimulation of an inflammatory tissue response resulting in collagen deposition.5 Each injection session with PLLA builds on the volumization achieved with the previous treatment. Once the final correction is achieved, it can persist for longer than 1 year, requiring a single treatment session for maintenance. The nonbiodegradable fillers provoke a foreign body reaction that stimulates a fibroblastic deposition of collagen around the nonabsorbable microspheres. Products in this category include polymethylmethacrylate (PMMA; Bellafill [Suneva Medical]); the polyacrylamide hydrogel Acquamid; and Silikon 1000, a medical-grade pure form of silicone. Bellafill (previously marketed as Artefill) consists of 80% bovine dermal collagen plus 20% PMMA microspheres. The collagen vehicle is degraded within 1 to 3 months, leaving the microspheres encapsulated by a fine fibrous capsule. Acquamid is a hydrophilic polyacrylamide gel composed of 97.5% sterile water bound to 2.5% cross-linked acrylamide polymer. A continuous exchange of fluid occurs between the hydrogel and surrounding tissue, which becomes integrated in the soft tissue.6 Silikon 1000 is injected in very small quantities using a microdroplet technique. Similar to the other permanent fillers, the body forms collagen around the silicone particles. The permanent nature of the nonbiodegradable fillers make their complications more long-lasting and difficult to treat. Any injection procedure has the potential to cause bruising. Bruising is related to several factors: • Filler used • Site of injection • Depth of injection • Size of the needle used to inject the filler • Amount of tissue trauma during injection • Patient’s propensity to bleed Bruising is observed more often after injection into the deep dermal and immediate subdermal planes using fanning and threading techniques, and less often when materials are injected using the depot technique at the preperiosteal level (Fig. 16.1). Larger-bore needles cause more trauma and more bruising. Cannulas are believed to produce less bruising than do sharp needles. Transcutaneous puncture sites should be limited, because each is a potential site of bruising, and tissue trauma should be minimized while “massaging and molding” the filler. Bruising can be further reduced by having patients avoid all anticoagulant medications for 5 to 7 days before the procedure (Box 16.1). The surgeon should contact the prescribing physician before instructing a patient to discontinue prescription anticoagulants and aspirin. The area to be treated can be cooled with ice packs and pretreated with local infiltration of lidocaine with epinephrine (using small volumes that will not distort the patient’s anatomy) for patients who have had problems with bruising after previous treatments. If local anesthetic is mixed with the filler, 2% lidocaine with epinephrine should be used. After the procedure, the application of cold compresses will limit bruising and swelling. The patient should sleep with the head elevated, and strenuous exercise should be avoided that day. Summary Box Most Common Problems with Dermal Fillers, Botulinum Toxins, and Deoxycholic Acid Treatment Complications Dermal filler Injection site trauma (bruising, erythema, edema) Noninflammatory nodules Inflammatory nodules Skin discoloration Infection Malar edema Botulinum toxin Injection site trauma (bruising, erythema, edema) Eyelid ptosis Eyebrow ptosis Lip asymmetry Deoxycholic acid Injection site trauma (bruising, erythema, edema, induration, pain) Injection site numbness Fig. 16.1 Bruising. • Aspirin • Warfarin • Dipyridamole • Clopidogrel • All nonsteroidal anti-inflammatory drugs • Fish oil • Vitamin E • St. John’s Wort • Garlic tablets • Gingko biloba • Ginseng If bruising occurs, the patient should avoid unprotected sun exposure as long as the bruising is present. Vitamin K cream has been shown to speed the resolution of ecchymosis, and persistent staining can be treated with pulsed-dye laser or potassium titanyl phosphate (KTP) laser and IPL.7 Immediately after injection some skin redness is normal. If erythema persists for more than a few days, the surgeon should consider hypersensitivity, other tissue reaction, or infection. A medium-strength topical steroid is advocated for persistent erythema. Long-term use of high-potency steroids should be avoided, because they may cause atrophy and telangiectasias. Treatments for rosacea may be effective, including oral tetracycline, metronidazole, and azelaic acid. Lasers and IPL can be effective for the treatment of telangiectasias and erythema (see later discussion). Vitamin K cream is useful in accelerating resolution of erythema and facial bruising.8 Patients with rosacea have a higher risk of developing postinjection erythema and should be warned of this before beginning the procedure. New capillaries, arterioles, and venules may occur at the site of dermal filler injection. These tiny vessels can appear days or weeks after the procedure but should fade within 3 to 12 months without further treatment. They are caused by tissue trauma as a result of tissue expansion by the product or by excessive molding and massage of the product. Lasers shown to be effective in the treatment of telangiectasias include 532-nm KTP, 532-nm diode copper vapor, 585-nm pulsed-dye lasers, and IPL. Darker skin has a tendency to hyperpigment after trauma.9 Dermal filler procedures are a common cause of postinflammatory hyperpigmentation in individuals with Fitzpatrick skin types IV through VI,10 although postinjection hyperpigmentation can also be seen in other skin types. If persistent hyperpigmentation develops after dermal filler injection, first-line treatment should be with a bleaching agent such as topical hydroquinone (2 to 8%) and tretinoin combined with daily full-spectrum sunscreen application. If this is unsuccessful, the next step is treatment with IPL, a pulsed-dye laser, or fractional laser; the low fluence Q-switched neodymium-doped: yttrium aluminum garnet (Nd:YAG) 1064-nm laser is also effective. Current lasers have limited use in the treatment of Fitzpatrick skin types IV to VI, but the long wavelength Nd:YAG laser allows darker skin to be treated without disrupting natural skin color, and IPL systems can treat Fitzpatrick skin types I to IV. Limiting the number of skin punctures during the injection process by using the linear threading or fanning technique or injecting at the preperiosteal level (“walking” the needle from depot to depot) may reduce injection trauma and resultant postinflammatory hyperpigmentation. When particulate HA fillers are inappropriately implanted into the superficial dermis or epidermis a bluish hue may occur as a result of the Tyndall effect (scattering of light by particles in suspension). Blue light waves have a higher frequency than red and are more easily scattered, so when a ray of light hits the skin’s surface and reflects off the super ficially placed particulate HA filler, it is reflected back with blue becoming the prominent reflected color. The more superficial the placement of any filler, the more visible it will be. Hyaluronidase should be the initial approach to treatment of HA visibility. For HAs that are less susceptible to hyaluronidase because of a high degree of cross-linking or large particle size, multiple treatments may be necessary (dosage is increased until material is dissolved). CaHA filler placed too superficially can be visible as white streaks or pustules or as salmon-colored discoloration of lower eyelid skin (Fig. 16.2). CaHA or HA can be treated by nicking the skin with a small-gauge needle (30 gauge) or surgical scalpel (no. 11 blade) and expressing the superficial unwanted dermal filler.11,12 This procedure can be performed immediately or as long as 12 months or more after placement.12 I have found this is only effective in the first 48 hours after injection with CaHA. As with any procedure that breaks the surface of the skin, dermal filler injections are associated with a risk of infection. This is exacerbated by the presence of the filler implant, which significantly reduces the threshold concentration at which contaminating bacteria can cause infection. To minimize this risk the injection site must be cleansed with an effective topical disinfectant (alcohol, povidine iodine, or preferably 2% chlorohexidine gluconate in 70% alcohol), the needle and syringe should be safely removed from the sterilized individual packaging, gloves should be worn throughout the procedure, and care should be taken that the needle is not contaminated during the procedure.13 Excess filler material should not be wiped from the needle tip with nonsterile gauze; residual amounts of material should be flicked off the needle. Injection sites should be cleansed again after manipulation with nonsterile gloves. Care must be taken to use strict aseptic technique when mixing or reformulating a product. Although rare, postfiller infections do occur and may be bacterial, fungal, polymicrobial, or viral. Virulent late infections (biofilms) can also occur. I believe that many filler adverse events, including nodules and persistent, fluctuating edema and erythema, are at least in part caused by bacterial contamination. Fig. 16.2 (a) Superficially placed Radiesse that resulted in contour irregularity and dyschromia. (b) Irregular placement of Radiesse with visible material causing irregular contours. (c) Salmon-colored discoloration after Radiesse injection into the infraorbital hollow and tear trough. Erysipelas and phlegmon are a diffuse inflammation of the skin or connective tissue caused by infection. As is the case with cellulitis and abscess, responsible organisms are usually Staphylococcus aureus or Streptococcus pyogenes, but gram-negative, anaerobic, and atypical infections have been reported.14 If untreated the conditions may lead to sepsis, particularly in elderly people and those with diabetes or other illnesses that alter the immune system. Mild forms may be treated with oral antibiotics, but more serious cases require intravenous antibiotics and hospitalization. Antibiotics with activity against S. aureus are necessary, such as cephalexin, dicloxacillin, doxycycline, or nafcillin. To avoid spreading infection, hyaluronidase should not be used in the primary phase, and the area should not be massaged. If the injectate was HA and a recurrence occurs after antibiotic treatment, hyaluronidase should be considered to eliminate any persistent nidus of infection. Abscesses should be treated with incision and drainage and antibiotics. Cultures should be obtained, if possible, before initiating antibiotic therapy. Treatment should then be tailored to the obtained sensitivity reports.15 Midfacial and periorbital infection can in rare cases result in intracerebral complications. Dermal filler injections can lead to reactivation of herpes virus infections. If the treatment is targeting the lips or mouth area and the individual has a history of cold sores, prophylactic treatment with valacyclovir (500 mg twice daily) immediately before and for 1 to 2 days after injection should be considered. If the patient has not received prophylactic treatment but infection is recognized early, valacyclovir at a dose of 2 g twice daily for 1 day should be given. If suprainfection occurs, the patient should be treated with appropriate antibiotics. Most herpetic recurrences occur in the perioral area, nasal mucosa, and mucosa of the hard palate. Shingles (herpes zoster) after injection is very rare. When a blistering reaction occurs outside of the areas of recurrent herpes simplex virus infection (lip skin and vermilion, nasal mucosa, and mucosa of the hard palate), a diagnosis of vascular compromise should be considered. Biofilms occur when injected filler material becomes contaminated with bacteria or yeast. This can take place at the time of injection, after injecting a patient previously injected with filler, after systemic infection or local infection, or after a procedure that causes a bacteremia (e.g., a dental cleaning). Biofilms are widespread in nature and consist of densely packed communities of bacteria that surround themselves with secreted polymers and are irreversibly adherent to a living structure or an inert surface. When a material is injected into the skin or subcutaneous tissue, it can become coated with bacteria and a biofilm can form. These complex collections of bacteria are very difficult to treat, so the focus should be on prevention. Initially, free swimming organisms attach to a surface. They achieve a permanent chemical attachment and secrete a protective and adhesive matrix of extracellular polymeric substance (EPS). Biofilm EPS, which is also referred to as slime, is a polymeric conglomeration generally composed of extracellular deoxyribonucleic acid (DNA), proteins, and polysaccharides. The microbial cells growing in a biofilm are physiologically distinct from planktonic cells of the same organism, which, by contrast, are single cells that may float or swim in a liquid medium. Over time the single layer becomes thicker, and vertical towers and horizontal channels develop. Once mature, a biofilm gives rise to a low-grade chronic infection that is resistant to antibiotics and difficult to culture.16,17 The matrix encases the cells within it and facilitates communication among them through biochemical signals and gene exchange. Bacteria in a biofilm may require higher antibiotic concentrations and transfer antibiotic resistance by sharing genetic material via plasmids. Bacteria within a biofilm shift between an active and dormant state, the former generating little host response and resulting in negative cultures. More sophisticated examination of biopsied tissue (fluorescence in situ hybridization using peptide nucleic acid probes) may be required for diagnosis. A mature biofilm will release individual free swimming bacteria in the tissues. Many bacterial species are capable of forming a biofilm. The most common organisms are S. aureus and Staphylococcus epidermidis, but Pseudomonas aeruginosa, Enterococcus species, and yeast and fungi (e.g., Candida) can also form biofilms. When activated, for example by trauma from a subsequent dermal filler procedure, the biofilm can cause a local infection, a systemic infection, or a granulomatous or inflammatory response. Distinguishing inflammation caused by a bacterial biofilm from a low-grade hypersensitivity reaction is difficult. If an erythematous and/or indurated area appears at any time after treatment, regardless of duration, a biofilm should be suspected.18,19 Persistent inflammatory conditions not showing improvement with other therapy and inflammatory nodules that recur after resolution may also indicate a biofilm. The signs of inflammation may be no more than edema with or without erythema and induration, or nodularity at the treated site (or a site that has been treated with filler before the most recent treatment). Because they are usually culture negative, these nodules were previously believed to be a result of an allergic or foreign body reaction to the filler substance. However, the technique of fluorescence in situ hybridization confirmed an infective cause in a series of polyacrylamide gel-related, culture-negative, inflammatory nodules.20 The use of scintigraphy with radiolabeled autologous white blood cells is also an accurate method for diagnosing infection in patients with long-term dermal filler complications.21 Most inflammatory nodules that are resected and sent for pathology are reported as foreign body granulomas, so the importance of biofilm as a cause of inflammatory nodules is still not quantifiable. A clinician’s index of suspicion for biofilm formation should be high, and biofilm should be at the top of the differential diagnosis when signs of inflammation occur weeks to months after a previously uncomplicated injection procedure. Antibiotic treatment is the first step in treating a patient with a suspected biofilm, even if the culture is negative, and should be initiated with a broad-spectrum agent (quinolone) such as ciprofloxacin 500 mg twice daily and a macrolide such as clarithromycin XL 500 mg twice daily for 3 to 6 weeks (see Fig. 16.6 later in the chapter). Combination amoxicillin and clavulanic acid, a cephalosporin, or doxycycline can be substituted for the macrolide. Single antibiotic therapy can be started if the index of suspicion is lower. I have patients continue antibiotics for 2 weeks after all signs and symptoms have resolved. If there is a suspicion of biofilm, intralesional steroids should not be used until antibiotic therapy has been initiated, because they can exacerbate the problem. With any biofilm, whether a result of a biodegradable or nonbiodegradable product, removal of the filler will reduce the inflammatory potential of the biofilm, because it is irreversibly adherent to it. Hyaluronidase should be used if the patient was injected with an HA. Because the biofilm EPS contains HA, hyaluronidase may be useful in the treatment of all biofilms. I also believe that in addition to antibiotics repeated injections of hyaluronidase should be performed when treating a biofilm where an HA filler was used before administering oral or intralesional steroids. The exact dosage necessary to dissolve the highly cross-linked HA fillers in use today has not been quantified (particularly because the exact location of the injected subcutaneous material cannot be accurately determined). Hyaluronidase must be in direct physical contact with its substrate to work. One or more intralesional steroid injections and/or courses of oral steroids may result in reduction of inflammation but make it difficult to make appropriate therapeutic decisions because the clinician cannot gauge the patient’s true response. Laser technology has been reported to have beneficial effects in the treatment of infectious filler complications.22 The intralesional subcutaneous introduction of an optic laser microfiber and the subsequent heat production result in a theoretical decrease of bacterial counts of the biofilm and in liquefaction of the filler microparticles. Radiofrequency heating has been used in the same fashion. These minimally invasive techniques could be an intermediate step before attempting surgical excision of an inflammatory nodule. • Thoroughly cleanse the area before injection • Reprep after contaminating the site • Avoid contaminating the filler or needle • Avoid injecting through oral or nasal mucosa • Avoid hydrophilic permanent materials • Avoid injecting over previous filler or into traumatized or infected tissue • Promptly and aggressively treat any postfiller infection The incidence of biofilms as a result of filler injections is not known, and diagnosis is difficult. Fortunately biofilms are very rare with most filler products, but it is important to take precautions to prevent infection when injecting fillers (Box 16.2). Some transient swelling in the immediate postprocedural period is normal and occurs with all dermal fillers. This type of edema occurs very shortly after injection and is related to the volume and technique used. It also appears to be idiosyncratic, because it occurs in some patients but not in others who have been treated using the same technique and filler. Methods for avoidance are the same as those for bruising (i.e., smaller needles, atraumatic technique, and avoiding overly vigorous massage of the treated area). Most cases of postinjection, trauma-related edema resolve without treatment within 7 days. Most require no treatment other than elevation of the treated site. In severe cases patients can be treated with a steroid dose pack, but the injector must be vigilant not to miss an infective cause. There are also some cases of edema that do not resolve within the first week after injection. These occur within hours to several days or weeks after the injection, may persist for months, and may or may not be confined to the site of injection. I group these cases by probable etiology based on temporal occurrence of the edema, the clinical appearance, and retrospectively what treatment the patient responded to. Acute hypersensitivity reactions to dermal fillers are very rare. Dermal fillers are essentially foreign bodies, and some patients may manifest hypersensitivity reactions to injected products because of an antibody-mediated (usually immunoglobulin E [IgE]) immune response (type I hypersensitivity reaction). This may occur after initial or repeated exposure. IgE stimulates mast cells to degranulate, releasing proteases, heparin, histamine, cytokines, prostaglandins, leukotrienes, and platelet-activating factor, which result in the edema, erythema, pain, and itching characteristic of an urticarial or angioedemic allergic response. One mechanism proposed for hypersensitivity associated with HA is its interaction with tissue resident mast cells through the CD44 receptor.23 Angioedema occurs within hours of exposure. Reactions can be severe and last for several weeks.24 Edema may be confined to the injection sites but may also be more generalized. An acute idiopathic allergic response can also occur in which no allergen can be identified. The reaction may be localized, or there may be acute generalized facial edema (Fig. 16.3). Fig. 16.3 (a) Acute generalized edema after Radiesse injection. (b) Delayed generalized edema occurring 7 days after injection of Voluma (Allergan) to the cheeks. (c) At 6 months after injection, the patient in (b) has persistent edema and moon face from oral steroid administration. Treatment of angioedema, whether of known cause or idiopathic, depends on the severity of the condition. In many cases the swelling resolves spontaneously after a few hours or days. If mast-cell mediated, the swelling is short lived and responsive to antihistamines (both H1 and H2, sedating and nonsedating). I have found that the most patients with filler-related edema do not respond to antihistamines and therefore are not demonstrating classic type I hypersensitivity reactions. For edema not responsive to antihistamines, oral prednisone is the mainstay of treatment (Fig. 16.4). The patient should be closely monitored to ensure the edema is not a result of an infectious process. Rapidly progressing angioedema is treated as a medical emergency because of the risk of airway obstruction and is treated with subcutaneous administration of epinephrine, antihistamines, and oral steroids. Chronic urticaria or angioedema refers to episodes that last more than 6 weeks. These cases are often difficult to treat and have a variable response to medication. When treating chronic urticaria from other causes, immunomodulators (cyclosporine, dapsone, methotrexate, mycophenolate, mofetil, cyclophosphamide, hydroxychloroquine, and sulfasalazine) have been used. The algorithm featured in Fig. 16.4 highlights the treatment steps recommended. Each step is added to the previous one if an inadequate response is obtained. Edema should be controlled with the smallest dose of oral steroids that is effective. I have had success in reducing the steroid dose with concurrent use of the leukotriene receptor antagonist montelukast, 10 mg per day. Delayed hypersensitivity reactions are characterized by induration, erythema, and edema and are mediated by macrophages and T lymphocytes (rather than antibodies) and may lead in many cases to the development of granulomatous inflammation. They typically occur 48 to72 hours after injection but may be seen as late as several weeks after injection and may persist for many months.25,26 Delayed hypersensitivity reactions are nonresponsive to antihistamines. The allergen should be removed (see Fig. 16.4). In the case of HA this will involve treatment with hyaluronidase. For other fillers this may involve treatment with steroids until the filler resorbs, laser treatment, and/or extrusion.22 Excision is a last resort. Symptoms should be controlled with the lowest possible dose of oral steroids (prednisone). Nodule development is a common adverse event after the use of fillers for soft tissue augmentation. They are commonly categorized as inflammatory or noninflammatory. Noninflammatory nodules are typically seen immediately or shortly after implantation and are usually secondary to improper placement of the filler. Inflammatory nodules can occur from days to years after filler placement and vary as to their cause. When too much material accumulates in an area as a result of poor technique (overcorrection, too superficial placement of a filler, or inappropriate placement into a structure, such as intramuscular placement in a sphincteric muscle) (Fig. 16.5), a noninflammatory nodule may result that is palpable and may be visible. Such implant nodules do not grow and are well delineated. They appear early after the procedure and should be differentiated from hypersensitivity reactions, foreign body granulomas, or biofilms, which are a result of an inflammatory reaction around the product or site of infection and usually occur later. Poor technique and filler placement and the use of particulate fillers (e.g., PMMA, CaHA) in highly mobile areas such as the lips can cause delayed-onset noninflammatory nodules.27 Fig. 16.4 Immune-mediated edema. HA, Hyaluronic acid; LMW, low molecular weight. If nodules occur after treatment with an HA filler they will resolve with hyaluronidase treatment. Early nodules occurring after treatment with a non-HA filler may respond to vigorous massage; the material can also be extruded (Fig. 16.6). Nodules may also be hydrodisrupted with lidocaine or saline followed by vigorous massage.28 The patient should maintain the disruption with home massage. Nodules that do not resolve may respond to intralesional steroids (keep intralesional and limit dose to avoid skin atrophy). Additional treatment options are a series of injections of 5-fluorouracil (5-FU), triamcinolone and lidocaine, or 5-FU and lidocaine. These can be repeated as long as improvement is noted. Fractional lasers, which are used after the carrier gel has been absorbed, have been reported to improve visible material in the lower eyelids and the lips after Radiesse injections.29,30 Excision of implanted material is only used as a last resort. Chronic, intractable nodules that persist for months despite disruption and become increasingly fibrotic are foreign body granulomas and should be treated as described in that section. Fig. 16.5 Noninflammatory nodules. (a) Juvéderm nodule in upper lip. (b) Juvéderm nodule in the lower lip. (c) Superficially injected Radiesse visible as a nodule in the lower eyelid. (d) Radiesse in the labial-gingival sulcus from mental crease injection. Implant nodules are one of the most common adverse events after dermal filler procedures,31 but their incidence can be reduced by taking care to maintain strict aseptic technique and to avoid too superficial placement of filler, selecting the appropriate filler for the tissue site, molding after injection to ensure even distribution and smoothness, avoiding intramuscular injection, and avoiding injection and particularly into sphincteric muscles (orbicularis oris and oculi) that may cause clumping of fillers. Inflammation around an implant particle is normal and always occurs and leads eventually to its resorption in the case of biodegradable fillers. Ideally such fillers should be immunologically inert and stimulate collagen neogenesis to allow persistence of the product and not initiate a granulomatous reaction. Phagocytosis by macrophages is an initial tissue reaction to any foreign body and is the most important factor in determining filler longevity. Circulating granulocytes are attracted to the site. Monocytes differentiate into macrophages that phagocytize particles that the polymorphonuclear cells cannot. Particle sizes greater than 5 μm resist degradation by macrophages. Activated macrophages secrete a variety of cytokines and other inflammatory products that attract additional macrophages and blood monocytes. Individual macrophages may become larger (epithelioid histiocytes) or fuse to form multinucleated foreign body giant cells. These cells are characteristic of granulomas, and if a biopsy is obtained, a true granulomatous reaction can be confirmed histologically. Particle shape, surface charge, and hydrophilicity also affect phagocytosis. In the case of HA and collagen fillers, cross-linking also inhibits phagocytosis. There are three potential causes for inflammatory nodules32: 1. Immune-mediated reactions (classic or direct) 2. Foreign body responses 3. Infectious processes Regardless of the cause, when a biopsy of an inflammatory nodule is performed histologic examination invariably confirms a diagnosis of a foreign body granulomatous response. Fillers have been suggested to act as T-cell–specific activators and adjuvants (rather than antigens) in individuals with predisposed genetic backgrounds.33 They may do so directly or in association with a biofilm. Inflammatory filler-related adverse events have also been linked to triggering factors such as local trauma, infections, or vaccine administration (potentially because of increased interferon levels). Another potential cause of inflammatory responses to Voluma and other HA fillers may be direct effects of HA fragments at the site of injection. HA is generally thought not to be immunostimulatory because it is found in the extracellular matrix of human and animal dermis and has no species specificity. However, a recent report documents a number of cases of delayed-onset nodules after treatment with Voluma, a volumizing HA filler.34 Delayed nodules were identified in 23 out of 2,342 (0.5%) patients treated over 68 months. The median time to onset of nodules was 4 months (range, 1 to 13 months), and the median time to resolution of the nodules was 6 weeks (range, 1 to 36 weeks). A seasonal variation in onset of nodules was also observed, with most occurring in the fall and winter. Nine of the patients (39%) had an immunologic stimulus such as a flulike illness or dental procedure immediately preceding the reaction. Fig. 16.6 Noninflammatory nodules. Initially, immune responses to HA fillers were proposed to be caused by impurities such as DNA fragments, endotoxins, and proteins in the filler left after their manufacture. Since these impurities have been reduced with improvements in the manufacturing process, the incidence of hypersensitivity reactions has diminished, but they still occur. Recent literature suggests that this may not be a result of the antigenicity of the filler, but rather its structural composition.35,36 High-molecular-weight fragments of HA (HMW-HA) are primarily anti-inflammatory, whereas low-molecular-weight fragments (LMW-HA) are proinflammatory and trigger the immune system. LMW-HA has been shown to inhibit fibrocyte differentiation via the CD44 receptor.35 An interaction with CD44 is also involved in LMW-HA–induced proinflammatory cytokine interleukin 6 (IL-6) and chemokines IL-8, CXCL1, CXCL2, CXCL6, and CCL8 gene expression in normal human dermal fibroblasts.36 LMW-HA can also activate macrophages, dendritic cells, and signal T cells (CD44 and TLR4). LMW-HA is present in Voluma and may increase in concentration as the product is metabolized after injection. This effect, alone or in combination with a triggering event, may produce a vigorous inflammatory response. This recent link to the nonantigenic immune stimulatory properties of HA is further evidence of our lack of understanding of the mechanisms of inflammatory dermal filler reactions. There may be other physical or chemical properties distinct to a particular filler or group of fillers, or their breakdown products that interact with the body to cause adverse reactions. The failure of effective phagocytosis leads to foreign body granuloma formation. The result is epithelioid histiocytes, foreign body giant cells, and a surrounding infiltrate of T lymphocytes that secrete cytokines such as tumor necrosis factor (TNF) alpha, interferon gamma, and IL-12, responsible for ongoing macrophage activation.33 Clinically, foreign body granulomas appear as red papules, nodules, or plaques (with or without ulceration) (Fig. 16.7). The center of the lesion may be necrotic, but any material expressed is usually culture negative. The lesions become firmer over time because of fibrosis. True foreign body granulomas are rare, with an estimated incidence between 0.01 and 1%. They can occur with all injectable dermal fillers and usually appear after a latent period, which can be several months to years after injection, as compared with 2 to 4 weeks for early noninflammatory nodules.37–40 Factors that influence increased foreign body granuloma development include the chemical composition of the filler, its hydrophilicity, surface charge, hyaluronic acid cross-linking, large injection volumes, intramuscular injection, and postinjection infections or facial trauma. The shape of the microspheres appears to be an important factor, with granulomatous reactions occurring less commonly after implantation of microspheres with smooth surfaces. Irregular and sharp-edged particles may induce more severe granulomatous reactions.41 Nonbiodegradable fillers are not characterized by a higher rate of foreign body granulomas than temporary fillers, but their clinical appearance is more pronounced and they persist longer if not treated appropriately. The development of foreign body granuloma can be delayed, coming as late as 1 to 2 years after treatment with polymethylmethacrylate microspheres and polyacrylamide. The structural changes that some nonbiodegradable fillers undergo during years in situ in human tissue may be one reason why adverse reactions to these permanent fillers occur clinically with a delay of several years.42 The mechanism of late inflammation or granuloma formation is still unknown. In some patients who have been previously injected with long-lasting or permanent filler and who have been asymptomatic (sometimes for many years), the injection of a second filler material at the same site triggers an inflammatory reaction against both fillers. Because the role of bacterial contamination and biofilms cannot as yet be quantified and they are responsible for at least some of these adverse events, the use of sterile technique for all stages of the procedure cannot be overemphasized. The skin should be cleansed of all makeup using an effective antiseptic (i.e., alcohol and chlorhexidine), and needle and skin contamination should be avoided when injecting. The same technique recommendations described previously for noninflammatory nodules apply to inflammatory nodules. Inflammatory reactions to HA fillers should be treated with hyaluronidase.43 It should be injected intralesionally, or for a more diffuse process throughout the site of filler injection. There are no specific dose guidelines, but an initial dose of 10 units per 0.1 mL of HA has been suggested.33,34 If inflammation improves but does not resolve, I have found repeated treatments with or without increasing the number of units to be beneficial. Others have recommended not using hyaluronidase in the presence of erythema and inflammation because of the potential for spreading infection. However, I believe that this risk is more than outweighed by the benefits of removing the substrate for a potential biofilm, the effect on the HA component of the potential biofilm EPS, and eliminating any immune stimulatory effects of the HA (either as an adjuvant, directly via LMW-HA, or as an antigen).
16
Dermal Fillers and Neurotoxins
Categories of Dermal Filler
Avoiding and Managing Complications Associated with Dermal Fillers
Bruising

Skin Erythema and Discoloration
Erythema
Neovascularization
Hyperpigmentation
Dyspigmentation
Infection

Erysipelas, Cellulitis, and Abscess
Herpetic Outbreak
Biofilms
Edema
Short-Term Posttraumatic Edema
Antibody-Mediated Edema (Angioedema)

Non–Antibody-Mediated (Delayed) Edema
Nodular Masses
Noninflammatory Nodules

Inflammatory Nodules
Immune-Mediated Delayed Nodules
Foreign Body Granulomas
Prevention of Inflammatory Nodules
Treatment of Inflammatory Nodules
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine