- •
Dermabrasion is an effective and economical modality to minimize the appearance of mild to moderate facial rhytids, especially around the mouth.
- •
Dermabrasion can be performed under local and topical anesthetics.
- •
Dermabrasion can be used to treat scars, age related rhytids, and rhinophyma.
- •
Pre-procedural preparation of the skin and patient education facilitates recovery and helps avoid complications.
- •
Avoid injury to the deep reticular dermis and beyond, this will result in scars.
- •
The best results are obtained in Fitzpatrick types I, II, and III skin with mild to moderate rhytids.
Introduction
Dermabrasion is an effective means of skin resurfacing that has withstood the test of time and still plays an important role in the approach to skin resurfacing and diminution of facial rhytids and scars be they from trauma, surgery, or acne. Laser resurfacing and chemical peels are very effective and remain the most popular means of skin resurfacing. Today, dermabrasion is commonly used for peri-oral rhytids, acne and other scars, and rhinophyma. Dermabrasion persists because it is effective, inexpensive, and straightforward to perform. It has the added benefit of more precise control of depth of dermal damage compared to other techniques.
Dermabrasion can be performed under local field anesthesia, nerve block, or general anesthetic. The equipment needed for dermabrasion is simple, inexpensive, and portable ( Figure 4.1 ). It consists of a base power unit, hand piece, and interchangeable heads or bits. This set up generates a controlled mechanical method to plane the epidermis and variable depths of the dermis. This mechanical and controlled injury to the dermis (on the shoulder of a rhytid or the raised portion of a scar) results in the new formation of collagen and neoepithelialization that is smoother or less prominant than pre-treatment. This requires careful patient selection, planning, and technical skill on the part of the operator.

Pertinent anatomy
Both fine and deep rhytids in the skin can be the result of sun damage, dermal atrophy, mimetic muscle activity, deflational changes in the face, smoking, and trauma. Changes associated with acne scars are also evident in the dermis. A basic understanding of the skin anatomy and structure is a prerequisite to understanding how dermabrasion works and how to perform it safely ( Figure 4.2 ). The skin is made up of three primary layers, the epidermis, dermis and hypodermis. The epidermis is the most outer layer of the skin, is keratinized for protection, non-vascular, houses the pigment forming melanocytes, and can be subdivided into five distinct layers.
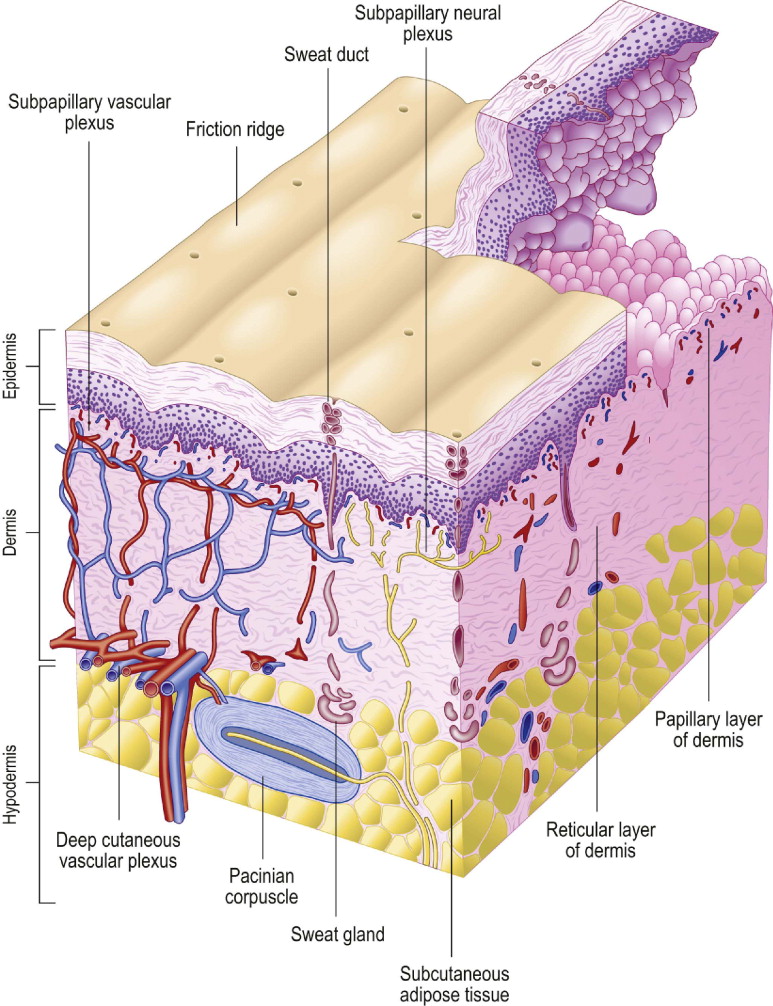
The dermis is the key component of skin as it relates to wound healing, skin strength, superficial blood flow in the skin, and the appearance of the skin surface. It is at this level that all skin resurfacing techniques have their effect. The dermis is subdivided into two distinct zones; the papillary layer and the reticular layer. The papillary layer is immediately deep to the epidermis and contains a dense collection of fine collagen fibers. Its superficial surface is marked by numerous papillae that interdigitate with recesses of the epidermis, marking the dermal–epidermal junction. Within this layer and the papillae are terminal capillary loops. The reticular dermis is deep to the papillary dermis, is thicker and contains collagen fibers that are coarser and thicker. The transition from fine to thick collagen fibers marks the papillary–reticular junction. At the base of the reticular dermis is a rich horizontally coursing blood supply.
The dermis is responsible for the regeneration of damaged epidermis. Stated differently and related to dermabrasion, a minimum amount of intact dermis is necessary to regenerate skin. If excessive dermal damage occurs, the ability to regenerate healthy dermis is compromised and scarring is more likely to result. One of the keys to successful dermabrasion is preserving a minimum amount of regenerative dermis so that fresh healthy skin results and not scar. The skin and other tissues of the face are privileged in that the robust blood supply enables adequate healing in response to significant dermal damage that would elsewhere heal with scar or not at all. It is the dermabrasion trauma that induces the skin regeneration process that results in the effacement of facial rhytids.
Patient evaluation and selection
Proper patient selection and assessment of the skin is critical to achieve a satisfactory outcome and avoid complications. A history is taken and a physical examination performed. A history of abnormal scarring, prolonged bleeding, delayed healing, tobacco use, medications, and use of topical skin care products is specifically reviewed. Patients taking isotretinoin (Accutane®) are at high risk for scarring from dermabrasion thus they are all instructed to stop taking Accutane prior to dermabrasion. Some dermatologists recommend at least 1 year cessation of Accutane before skin resurfacing.
It is also very important to review any previous ablative skin resurfacing or laser hair removal as these procedures also diminish the skin’s regenerative capacity. The location and depth of facial rhytids and presence of scars are noted. The Fitzpatrick skin type is identified (Fitzpatrick 1988). Type I skin is white, always burns and never tans; type II skin is white, usually burns, and sometimes tans; type III skin is white, sometimes burns, and usually tans; type IV skin is moderate brown, rarely burns, and tans easily; type V skin is dark brown, very rarely burns, and tans very easily; type VI skin is dark brown, never burns, and always tans. Peri-oral rhytids can also be classified; type I are mild and superficial usually sparing the lower lip, type II are moderate depth and extend across up to two-thirds of the upper lip with less extensive lower lip involvement, and type III rhytids are deep and thick involving the entire upper lip and lower lip including the chin.
Fitzpatrick types I, II, and III patients are well suited for dermabrasion but treatment of types IV, V, and VI should be avoided because of the increased risk of scar hypertrophy and hypopigmentation. All types of peri-oral rhytids can be treated, each requiring a different depth of injury. The delicate skin around the eyelid should not be treated with dermabrasion. Rhinophyma remains an excellent indication for dermabrasion as the treatment of choice. A history of previous skin resurfacing (laser or chemical peel) is a caution to the operator that less aggressive dermabrasion be performed.
If there is any question of the potential for poor healing or scar formation, a pre-procedural skin test can be performed easily in clinic. A small test patch of skin is chosen (usually behind the ear or other discreet area); it is anesthetized, then dermabrasion can be performed either with the formal set up or a sterile bovie scratch pad over a small area of skin. The patient is then followed closely. If normal healing occurs you can expect that dermabrasion can be done safely. If poor healing, scarring, or hypertrophy occur, dermabrasion should not be done and another less invasive method of skin resurfacing should be considered.
Indications
Dermabrasion is indicated for the reduction of the appearance of facial rhytids, acne scars, surgical scars, and treatment of rhinophyma. The most common facial rhytids still treated with dermabrasion are peri-oral lines. Patients who respond best to this treatment modality are the Fitzpatrick skin type I and II patients with mild to moderate facial rhytids.
Pre-operative preparation
Setting appropriate patient expectations, a description of the recovery experience, informed consent, and pre-operative skin care are all important. Patients are told that rhytids can be ‘softened’ and that they should not expect lines to be totally eliminated. The possibilities of complications such as scarring, permanent pigment loss, and prolonged recovery are discussed. All patients are pre-treated with a standard skin care regimen used prior to skin resurfacing. This includes topical tretinoin (Retin A®) and a hydroquinone based bleaching cream. The Retin A prepares and thickens the skin so recovery time is shortened and the bleaching cream pre-treatment helps minimize the pigment cell activity afterwards. Any supplements, vitamins, or medications that increase bleeding times or have anti-coagulant properties are stopped at least 1 week prior to the procedure ( Table 4.1 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


