Introduction
The deltopectoral (DP) fasciocutaneous flap, also known as the Bakamjian flap, is an important reconstructive tool that has been used for a wide variety of reconstructive problems in head and neck surgery. A variation of this flap that is based on a single perforator of the internal mammary artery is called the “internal mammary artery perforator (IMAP) flap.” The DP flap was initially described for facial reconstruction and resurfacing, as it was found to have an excellent color and thickness match to the native facial skin. In addition, the tissue from this region is thin and pliable, with the potential to provide a large area of well-vascularized tissue that is easily contoured.
This flap was first described in 1917 by Aymard for nasal reconstruction. In the 1930s, Joseph described this flap for head and neck reconstruction. However, it was not until the 1960s that this flap came to be used on a routine basis in head and neck reconstruction. In 1965, Bakamjian described the use of the medially based DP flap in the reconstruction of the laryngopharyngectomy defect, and the DP flap became the “workhorse” flap for resurfacing mucocutaneous defects of the head and neck.
With proper planning, as well as delay techniques in select circumstances, the DP flap can be used for reconstruction of any part of the anterior head and neck below the zygoma. The DP flap has been used in a variety of settings, including, but not limited to, closure of dehiscent wounds and fistulas, restoration of compromised regions including irradiated head and neck defects, and reconstruction of pharyngeal defects. Furthermore, reconstruction of complex head and neck surgical defects may require multiple flaps, and the DP flap may obviate the need for multiple microvascular free flaps. For some time now, the pedicled form of the DP flap has been largely overshadowed by the development of highly reliable regional flaps and the expanded use of free tissue transfer for head and neck reconstruction. Despite these trends, the DP flap remains a reliable option for the head and neck surgeon.
Flap Anatomy (see Fig 11.2 , Fig 11.3 , Fig 11.8 , Fig 11.9 )
This flap is based on the parasternal fasciocutaneous perforating branches of the internal mammary artery, which perforate the intercostal muscles and the pectoralis muscle to reach the skin. The blood supply to the anterior chest wall comes from perforators from the internal mammary artery that traverse each intercostal space; branches of the thoraco-acromial artery; musculocutaneous branches that traverse the deltoid muscle; the posterior intercostal vessels that give off perforators to the posterior, lateral, and anterior thoracic skin; and minor contributions from the lateral thoracic artery.
Arterial Supply of the Flap (see Figs 11.2 and 11.3 )
Dominant:
second or third perforating branches of the internal mammary artery
Length: 1.5 cm (range 1–2 cm)
Diameter: 1 mm (range 0.8–1.2 mm)
The internal mammary artery (IMA) branches off the subclavian artery.
- •
The IMA diameter of 1–2 mm; accompanying vein diameter of 2–3 mm
- •
Terminates into the musculophrenic and the deep superior epigastric arteries at the sixth intercostal space
- •
At each intercostal space, the IMA has three branches:
- •
Medial branch, which supplies the sternum
- •
Lateral branch, which communicates with the anterior intercostal artery
- •
Anterior branch, which supplies this flap.
- •
The anterior branch pierces the intercostal muscles and the pectoralis fascia running toward the skin. This vessel travels superficial to the fascial covering of the pectoralis major and deltoid muscles and terminates approximately 12 cm from the midline at the anterior axillary line.
- •
The caliber of this perforator ranges 0.5–1.2 mm.
- •
The second and third perforators are usually the largest caliber and run with their associated veins in the intercostal interspaces approximately 1–1.5 cm lateral to the border of the sternum.
- •
The flap is usually based on these large second and third perforators, but can be based on a single vascular pedicle in situations where a clearly dominant perforator is present.
- •
- •
Minor:
first and fourth perforating branches of the internal mammary artery (see Figs 11.2 and 11.3 )
Length: 1.5 cm (range 1–2 cm)
Diameter: 0.7 mm (range 0.5–1.2 mm)
Minor:
direct cutaneous artery that arises from the thoracoacromial system
This artery supplies a small area of skin below the lateral aspect of the clavicle overlying the deltopectoral groove.
Minor:
intercostal perforators
Some of the intercostal vessels send perforators that supply the skin of the anterior chest.
Venous Drainage of the Flap (see Fig. 11.8 )
Primary:
venae comitantes of the perforators from the internal mammary artery
Length: 1.5 cm (range 1–2 cm)
Diameter: 2.5 mm (range 2–3 mm)
The venae comitantes drain into the internal mammary vein, which subsequently drain into the innominate vein.
Secondary:
branch of the thoracoacromial vein
This branch could be used potentially to augment the venous drainage of a free DP flap.
Secondary:
cephalic vein
The cephalic vein runs in the deltopectoral groove between the axial pattern and the random pattern of the DP flap. Drainage through this vessel is presumed to improve blood flow of the distal DP flap.
Flap Innervation (see Fig. 11.9 )
Sensory:
the supraclavicular nerves of C3 and C4, and the anterolateral intercostal nerves of T2, T3, and T4 (see Figs 11.2 and 11.9 )
Motor:
this flap does not have a muscle component.
Flap Components
This flap is harvested as a cutaneous or a fasciocutaneous flap. Although not necessary for flap survival, the fascia overlying the pectoralis major muscle is often included with the flap harvest, for the purpose of protecting the nutrient blood supply. There is not a reliable source of bone that can be harvested with this flap.
Advantages
- •
The anatomy is reliable, and flap harvest is relatively easy.
- •
There is no need for additional patient positioning or preparation when dealing with defects in the head and neck or anterior part of the body.
- •
There is very little donor site morbidity and no significant functional deficits. The donor defect is easily covered by clothes.
- •
The fasciocutaneous flap is thin and pliable.
- •
The lack of a bulky muscular component makes it an excellent choice for replacing cutaneous defects.
- •
The skin of the flap matches the color and texture of the face.
- •
The flap size can be increased if a “delay” procedure or tissue expansion is performed.
- •
Two symmetrical DP flaps can be simultaneously harvested, effectively enlarging the available skin.
- •
The arc of rotation can be extended by removing a portion of rib and dissecting out the internal mammary artery.
- •
The effective pedicle length can be increased through modification referred to as the deltopectoral island flap (see below).
- •
This flap can be used even if a patient has had a pectoralis major flap if care was taken not to cut into the deltopectoral skin, and the internal mammary perforators were protected during harvest of the pectoralis flap (see Fig. 34.5 ).
- •
The DP flap can be used as a large migrating tube flap (“waltzing”).
Disadvantages
- •
Skin grafting of the donor site may be necessary if the harvest includes more than four interspaces or about 8 cm of skin. However, skin laxity in certain individuals may allow for more extensive donor defects to be closed primarily.
- •
Distal flap necrosis can occur when the skin paddle is extended over the deltoid region without a delay procedure.
- •
For some patients, hirsute skin can be an issue.
- •
In female patients there is the morbidity of chest skin scarring as well as the potential for alteration in breast symmetry and positioning or nipple distortion.
Flap Design
Anatomic Landmarks
- •
The lateral edge of the sternum ( Fig. 35.1 ) marks the medial aspect of the flap, the clavicle marks the superior aspect of the flap, the lower aspect of the 4th rib denotes the inferior aspect of the flap, and the lateral aspect of the flap, without a delay procedure, is 3–4 cm lateral and parallel to the deltopectoral groove.
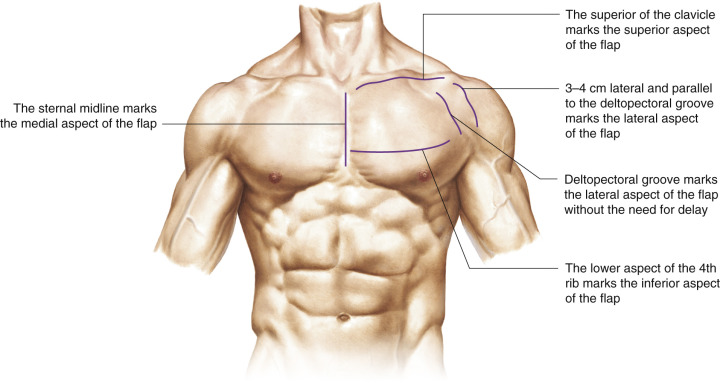
Figure 35.1
Anatomic landmarks.
- •
The superior and inferior limits of the flap may be adjusted based on the perforator chosen.
- •
The flap can be centered over one perforator, preferably the largest (the second or third perforator).
General Thoughts about Flap Design
- •
A handheld Doppler probe can be used preoperatively to detect the exact location of the perforators and the relative size of each perforator.
- •
The zone located 2 cm lateral to the border of the sternum should not be violated during harvest of this flap in order to avoid injury to these nutrient vessels.
- •
The flap can be designed based on any of the internal mammary perforators and oriented in a lateral, oblique, or inferior direction. The lateral direction toward the acromial process allows for the furthest extension of the flap, whereas the other two designs are limited in length unless a delay is performed.
- •
The DP flap can be raised and transferred in the primary setting with a high degree of reliability, provided that it does not include an extended territory overlying the deltoid muscle.
Angiosome Concept
The lateral extent to which the DP flap can be safely extended is of great importance in determining the utility of the flap for a particular defect and the safety of performing a one-stage reconstruction. In reviewing the vascular territory of the upper chest, it is apparent that vascular compromise, leading to distal flap ischemia, may occur when extending this flap to include skin overlying the deltoid muscle. Applying the angiosome model to this discussion, the primary region supplied by the internal mammary perforators includes the skin extending from the lateral border of the sternum to the deltopectoral groove. This area also receives musculocutaneous perforators arising from the thoracoacromial system and the pectoralis major muscle.
In the process of raising the skin flap over the deltoid muscle (beyond the deltopectoral groove), these musculocutaneous and direct cutaneous vessels are disrupted and the blood supply relies exclusively on the internal mammary perforating vessels, which transforms this distal region into a random pattern flap. In the angiosome model described by Taylor and Palmer, the blood supply to skin in immediately adjacent angiosomes is usually quite reliable. However, as one moves to the angiosome next in line or “once removed” from the source vessel, the pressure gradient of the nutrient flow diminishes. The skin overlying the deltoid muscle is an “angiosome once removed” from the internal mammary angiosome and, therefore, this skin is at risk for partial or total necrosis. Daniel et al. felt that if these lateral and posterior deltoid regions are to be incorporated in the flap harvest, it should be done following a delay procedure, to reduce the risk and subsequent morbidity of distal flap necrosis.
Special Considerations
The DP flap is a medially based axial flap with limited arc of rotation. The body habitus of the patient may influence the reach and therefore the utility of this flap. For example, a patient with broad shoulders and a short neck is a favorable scenario that expands the versatility of this flap.
Several different techniques with respect to flap geometry have been described. In discussing these variations, it should be kept in mind that one of the main problems with the DP flap is the potential for distal flap necrosis, which is due to the intrinsic limitations of the blood supply to this flap, as previously described.
Difference in Design, If Any, When Performing the Flap as Pedicled or Free
- •
The pedicled version of the flap usually includes more than one perforator from the internal mammary artery.
- •
During the harvest of the DP flap as a free flap, the branch of the thoracoacromial vein or the cephalic vein can be included in order to provide additional venous drainage if necessary. This would require the performance of venous anastomosis to a recipient vein in the neck.
- •
For both pedicled and free flaps, the pedicle length can be extended by dissecting the internal mammary vessels more proximally.
Flap Dimensions
Skin Island Dimensions
Length: 25 cm (range 10–30 cm)
Width: 8 cm (range 6–12 cm)
Maximum to close primarily: 5–9 cm
Primary closure of the donor site can be achieved if the flap is <5–6 cm, or 8–9 cm in elderly patients with lax skin. The medial and lateral aspects of the donor site are the most difficult to close primarily. Even if skin grafting is necessary, this can usually be limited by wide undermining and the use of retention sutures if necessary.
Flap Markings
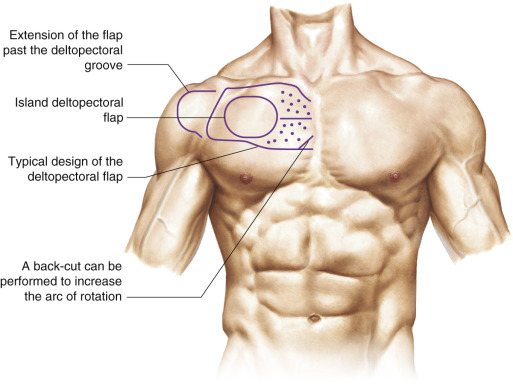
The flap is generally marked with a line parallel to the clavicle and centered over the second or third intercostal space or both ( Fig. 35.2 ), depending on the width necessary. The flap is extended in the direction of the acromion to the deltopectoral groove and beyond if a delay procedure is performed. The length can be extended 6–8 cm beyond the deltopectoral groove with a delay procedure.
Technique of Flap Harvest
The flap is harvested by extending the incision through the dermis and subcutaneous layers to the pectoralis fascia. Typically, the fascia is then incised and thus incorporated on the undersurface of the flap. This helps to preserve the perforating blood vessels that travel superficial to this fascial layer. The initial description of the harvest by Bakamjian described a subfascial dissection in order to preserve the flap blood supply. The flap should be elevated in this plane from a lateral to medial direction, with extreme care taken to stay at least 2 cm from the lateral border of the sternum.
Several different designs have been described for the DP flap. Traditionally, the flap is raised and transferred in the primary setting and does not require a two-stage delay procedure. The skin between the defect and the donor site can be excised, allowing for one-stage inset of the entire flap. Alternatively, the intervening skin bridge can be left in place with the DP flap tubed and exteriorized over the clavicle and neck skin. This technique then requires a second procedure to excise or return the pedicled component.
Deltopectoral Island Flap
The deltopectoral island flap is designed and harvested by detachment of the parasternal portion of the DP flap. This modification allows for a free axis of rotation (up to 180°), additional flap length, and improved spatial orientation capabilities. The flap is centered over the second intercostal perforator and is harvested as a traditional DP flap, with the additional parasternal elevation and detachment providing the island modification. The deltopectoral island flap is less tethered at the parasternal region, and the increased mobility and freedom of orientation allow for less tension on both the flap and the pedicle, stabilizing the flap and reducing the risk of vessel kinking with head movement. In addition, the proximal segment of the flap can be de-epithelialized and tunneled underneath the cervical skin between the defect and the clavicle. This maneuver allows for improved flap mobility and rotation and therefore greater versatility.
Chen et al. described the use of the Bakamjian island flap for patch esophagoplasty of the cervical esophagus. This island flap was used on 12 patients who had short segment esophageal strictures, with successful resumption of oral nutrition in all patients. An additional advantage described by Portnoy and Arena is the ability to incorporate the flap into closure of the donor site, allowing for primary closure and avoidance of skin grafting the donor site.
Split Deltopectoral Flap
Krizek and Robson described the vertically split DP flap that provides two epithelial surfaces. In this design, an incision is made along the longitudinal axis of the flap through the distal end of the skin paddle. This design allows for two separate segments that can be used for inner and outer lining restoration. This modification is safer, with respect to distal flap vascularity, than de-epithelializing a distal segment and folding the flap over on itself. This latter technique of a transverse fold at the distal segment of the flap creates more risk for vascular compromise as it requires a longer flap to be harvested, as well as placing the fold at the distal, less reliable portion of the DP flap.
L-Shaped Deltopectoral Flap
Another technique used to obtain an inner and outer lining is the two-stage L-shaped DP flap described by Bakamjian. In the first stage, the short limb of the “L” extending down along the upper arm was elevated and folded under the deltoid component to produce a buried skin flap. The two epithelial surfaces were then transferred at the time of the second procedure.
Two-Layered Deltopectoral Flap Provided by Skin Grafting the Undersurface
Another alternative solution to the requirement for a double epithelial surface is the use of a skin graft on the undersurface of the flap. The graft may be buried at the time of an initial delay procedure.
Fenestrated Flap
East et al. described the placement of a fenestration in the distal portion of the DP flap for reconstruction of a tracheostoma. In using this technique, the surgeon must be mindful of the possibility of distal tip necrosis. However, the authors advised that the short arc of rotation required to reach the tracheostoma allows the design of a short flap, and therefore the fenestra can be placed in a proximal, well-vascularized segment of the flap.
Free Microvascular Transfer of the Deltopectoral Flap
The DP flap has also been used as a microvascular free flap, first described in 1974 by Harii et al. The base of the free DP flap is located over the perforating branches of the internal mammary vessels parasternally; the upper border corresponds to the clavicular line and the lower parallels the upper and extends laterally across the apex of the anterior axillary fold. The base of the free flap is designed with the second perforating branch located along its midline. As with other free fasciocutaneous flaps, it has greater versatility than the conventional pedicle flap, and staged procedures are avoided. The DP flap provides an ample source of good quality skin suitable for facial reconstruction. Unlike the pedicled DP flap, which will not reach much beyond the zygomatic region, the free flap can be used for defects located throughout the head and neck region.
Fujino et al. described the transfer of a de-epithelialized dermis–fat flap for augmentation of contour deformities of the head and neck. The flap can be harvested as a free flap using the internal mammary perforators. However, the small caliber of these vessels, coupled with the short length of the vascular pedicle, render the revascularization technically difficult. It is technically feasible to anastomose vessels of this caliber, but the tenuous nature of this revascularization process has yielded a high incidence of anastomotic failure. Sasaki et al. were able to achieve improved reliability of the DP free flap by incorporating a segment of the internal mammary vessel in the vascular pedicle. In their experience, the caliber of the internal mammary perforators ranged 0.6–1.2 mm, with an average of 0.9 mm. However, if a segment of the internal mammary artery was used, the average size was 2.1 mm, with the vein averaging 2.9 mm. In addition, there was another 2–3 cm gained in pedicle length, which greatly facilitates the revascularization process and improves flap reliability.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


