CHAPTER 20 Deep plane procedures in the neck
Introduction
The cervicomental angle and the contours of the neck are very important determinants of facial aesthetics and are readily modified in facial rejuvenative surgery. Deep plane procedures in the neck are often required to reach the aesthetic endpoint of a defined, less obtuse cervicomental angle and smooth surface contours. Four structures are altered in deep plane procedures of the neck: the platysma, subplatysmal fat, the anterior belly of the digastric muscle, and the submandibular gland. Deep plane procedures involving these structures are most effective when employed in concert with other rejuvenation efforts in the superficial structures of the neck and the remainder of the face. With that in mind, this chapter focuses on deep plane procedures and how they are integrated into a global approach to cervicofacial rejuvenation.
Physical evaluation
• The first step in evaluation for the neck is a visual inspection. The front view is helpful in identifying platysmal bands and the lateral view permits assessment of the configuration of the cervicomental angle (Fig. 20.1).
• Visual inspection and palpation are performed to assess skin quality and skin excess. Sun-damaged skin, inelastic skin and skin with a crepe-like quality will likely require more excision in the postauricular region to facilitate envelope redraping (Fig. 20.2).
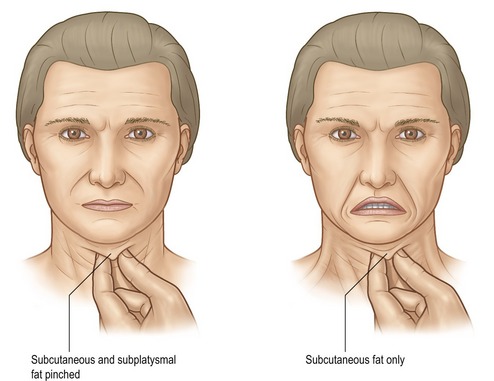
• The patient is instructed to flex her platysma muscle to accentuate the visibility of bands (Fig. 20.3). The submental region is palpated with the thumb in opposition to the fore and long fingers before and after activation of the platysma in order to differentiate subplatysmal bulk (anterior belly of the digastric muscle and fat) from preplatysmal fat (Fig. 20.4).
• With the head in the neutral position (Frankfort horizontal parallel to the ground) the bulk in the region of the anterior belly of the digastric muscle is visualized and palpated.
• Thyroid cartilage position and prominence are noted and are important to consider in female patients in whom a platysmal myotomy is planned. The myotomy is planned sufficiently low (2 cm below the cartilage) so that the thyroid cartilage prominence is not unmasked, thus producing a masculine appearance.
• The submandibular triangle is inspected by palpation for a discrete firm mass that can often be balloted against the medial and/or caudal surface of the body of the mandible. When such a mass is appreciated, the submandibular gland is hypertrophic and/or ptotic and excision may be considered to improve the neck contour.
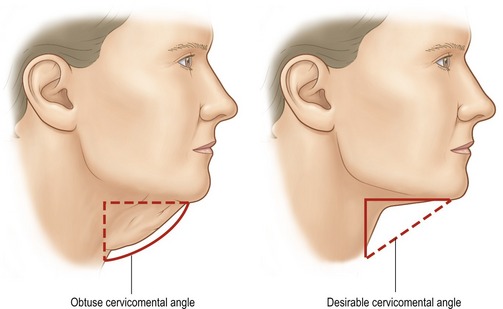
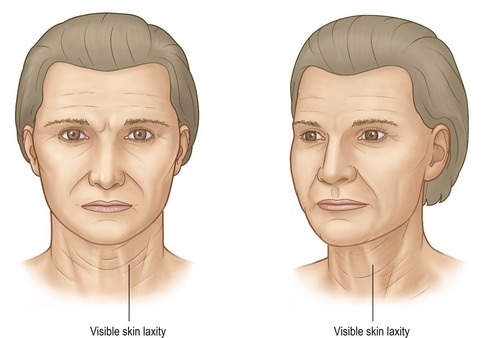
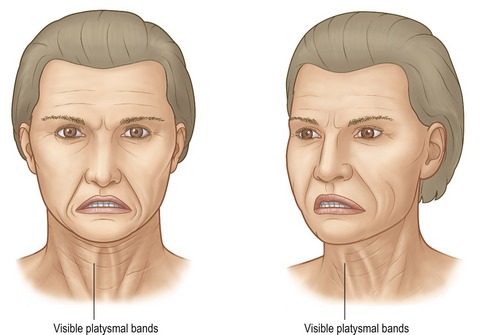
Fig. 20.3 Physical exam. The middle figure demonstrates cervical animation to identify platysmal bands.
Anatomy
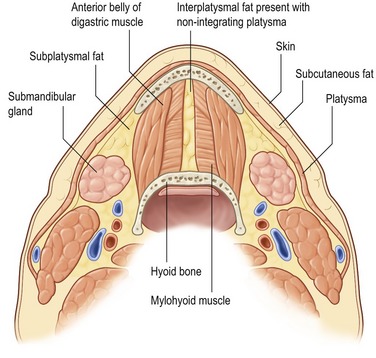
Procedures on the neck are designed to modify the submental/submandibular regions and the cervicomental angle regions by reduction and/or relocation of volume. The excess volume exists in three planes: the superficial plane between the skin and platysma, the intermediate plane comprised of the platysma and interplatysmal fat lying between the bilateral medial platysma edges, and the deep plane beneath the platysma containing the subplatysmal fat, the anterior belly of the digastric muscles, and the submandibular glands.
The platysma muscles are thin bilateral structures that extend from the SMAS in the face to the clavicles. There are three variations of platysmal anatomy in the submental region (Fig. 20.5):
• Type I (75%): Interdigitation of the plastysma muscles to a point 1–2 cm posterior to the mandibular symphysis.
• Type II (15%): Interdigitation of the plastysma muscles from the mandibular symphysis to the thyroid cartilage.
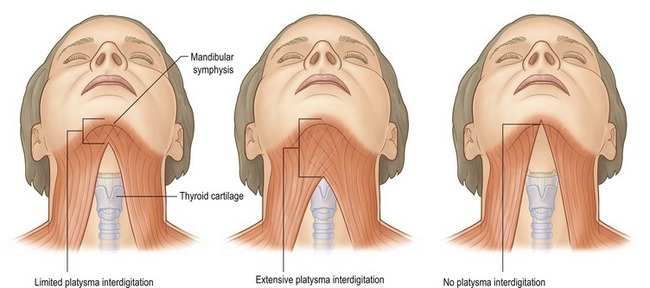
In patients with minimal to no plastysmal interdigitation, interplatysmal fat is found in the submental region between the medial edges of the two platysma muscles. This interplatysmal fat is considered a structure of the intermediate plane, but is contiguous with the subplatysmal fat of the deep plane. In those with complete interdigitation (no platysmal decussation) there is no interplatysmal fat and the fat referred to as “subplatysmal fat” is located deep to the plastysma, superficial to, between, and lateral to the anterior bellies of the digastric muscles.
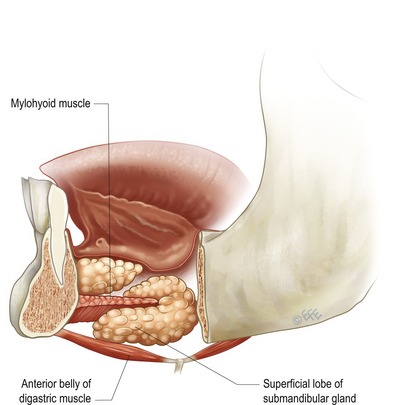
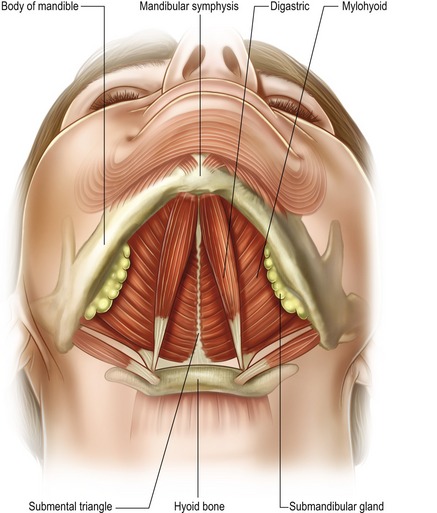
The anterior bellies of the bilateral digastric muscles may be hypertrophied or more visible in some patients resulting in excess submental bulk. These muscles are paired bilateral structures that extend between the lesser cornu of the hyoid bone and the posterior surface of the mandible on either side of the symphysis (Fig. 20.6). Each anterior belly forms one side of the bilateral submandibular triangles. The other two borders of the submandibular triangles are the posterior belly of the digastric muscle and the inferior edge of the body of the mandible. These triangles contain the submandibular gland, facial artery and vein, lingual nerve and the marginal mandibular branch of the facial nerve. Motor innervation of the anterior belly of the digastric muscle is a branch of the mandibular division of the trigeminal nerve. The muscles function as week depressors of the mandible. Excision proceeds without noticeable alteration in function.
The submandibular gland, a salivary gland, may produce a visible bulge in the region of the submandibular triangle, when it is hypertrophied and/or ptotic (Figs 20.7, 20.8). This bulge disrupts the otherwise planar surface that typifies the smooth contour of a youthful appearing neck. The facial artery and vein run obliquely over the posterior portion of the gland and the marginal mandibular can run horizontally across the superior aspect of the gland in a plane just superficial the facial artery and vein. Both the lingual nerve and the hypoglossal nerve lie deep to the gland. These vascular and neural structures are located in an extracapsular location, thus intracapsular resection of the gland is one strategy to reduce the risk of excessive bleeding and nerve injury.