Patients’ desires for aesthetics treatments that are safe, effective, and longer lasting have shaped innovation in BotulinumtoxinA (BoNTA). Daxibotulinumtoxin A (DaxiBoNTA), recently approved by the Food and Drug Administration in 2022, contains a synthetic stabilizing excipient that improves efficacy and extends duration. The potential advantage of fewer treatments coupled with its superior diffusion and rapid onset has led many patients and clinicians to consider transitioning to this BoNTA. This article highlights the differences between commercially available BoNTA’s, Daxi-BoNTA’s physical attributes that contribute to its favorable clinical profile, and the indications, methods, and considerations for transitioning patients to this new BoNTA.
Key points
- •
The synthetic stabilizing excipient of daxibotulinumtoxin A (Daxi-BoNTA), RTP004, contributes to its improved efficacy, diffusion, and extended median duration of 24 weeks, as reported in clinical trials.
- •
Daxi-BoNTA’s optimal diffusion allows for an even, “field effect” most beneficial when treating broad muscles such as the frontalis and orbicularis oculi.
- •
Patients transitioned from other botulinumtoxin A (BoNTA) due to suboptimal response tend to show superior results with Daxi-BoNTA.
- •
For upper facial lines and platysma, 1U of onabotulinumtoxin A (Ona-BoNTA) approximately equals 2U Daxi-BoNTA; for lower facial lines, IU of Ona-BoNTA approximately equals 1.5U Daxi-BoNTA.
- •
Recommended Daxi-BoNTA dosing for the lower facial lines and platysma are off-label and based on clinical observation, as no clinical trials data currently exist.
Video content accompanies this article at http://www.advancesincosmeticsurgery.com .
Introduction
The landscape of esthetics has and continues to transform at an accelerated rate. Informed by patients’ needs, innovation has led to the creation of safer, more effective, and longer lasting products. The first botulinumtoxin A (BoNTA), onabotulinumtoxin A (Ona-BoNTA), was approved by the Food and Drug Administration (FDA) in 2002 for the treatment of moderate-to-severe glabellar lines (GL). During the span of 2 decades, new BoNTAs have entered the market, each with unique physical attributes that often translate to specific benefits in clinical practice. To date, the FDA has approved 4 more BoNTAs for the treatment of moderate-to-severe GL: abobotulinumtoxin A (Abo-BoNTA) in 2009, incobotulinumtoxin A (Inco-BoNTA) in 2010, prabotulinumtoxin A (Pra-BoNTA) in 2019, and, most recently, daxibotulinumtoxin A (Daxi-BoNTA) in 2022.
This article will introduce and discuss the differences between commercially available BoNTAs, with specific focus on the physical and clinical attributes of Daxi-BoNTA, as well indications, methods, and considerations for transitioning patients to this new BoNTA.
Botulinumtoxin A: what are the differences?
Core Neurotoxin and Accessory Proteins
In its natural form, BoNTA is produced by the bacterium, Clostridium botulinum . In humans, BoNTA’s light chain binds to synaptosomal-associated protein 25 on the presynaptic membranes of neurons, preventing the release of the neurotransmitter acetylcholine, resulting in muscle paralysis.
All commercially available BoNTA contain an identical core 150 kDa (kilodalton) neurotoxin isolated from C . botulinum. Differences in BoNTAs lie entirely in their patented manufacturing process [ ]. Specifications of protein purification, stabilization, and excipients added during production determine the distinctive physical properties of BoNTAs and render important differences in their clinical application ( Table 1 ). Understanding how these differences influence the clinical profile of each BoNTA formulation allows clinicians to tailor treatments to their specific patient’s needs.
| Generic Name | OnabotulinumtoxinA | AbobotulinumtoxinA | IncobotulinumtoxinA | PrabotulinumtoxinA | DaxibotulinumtoxinA |
|---|---|---|---|---|---|
| Brand Name | Botox | Dysport | Xeomin | Jeuveau | Daxi, Daxxify |
| Indications | GL, LCL, FHL Approved: 2002, 2013, 2017 | GL Approved: 2009 | GL Approved: 2010 | GL Approved: 2019 | GL Approved: 2022 |
| Manufacturer | Allergan, Inc | Ipsen | Merz Pharmaceuticals | Evolus | Revance Therapeutics, Inc. |
| Active Substance (Molecular Weight) | BoNTA + AP (900 kDa) | BoNTA + AP (500–900 kDa) | BoNTA (150 kDa) | BoNTA + AP (900 kDa) | BoNTA (150 kDa) |
| Nanogram of toxin (per dose) | 0.18 ng/20U | 0.27 ng/50U | 0.08 ng/20U | Unknown | 0.18 ng/40U |
| Excipients | HSA Saccharose Sodium chloride | HSA Lactose | HSA Sucrose | HSA Sodium chloride | RTP004 a Polysorbate-20 (surfactant) Sugar Buffer |
| Purification method | Crystallization | Chromatography | Chromatography | Not available | Chromatography |
| Finishing method | Vacuum-drying | Lyophilized/freeze dried | Lyophilized/freeze dried | Vacuum-drying | Lyophilized/freeze dried |
| Potency testing method | Cell-based assay | Animal-based (LD50) assay | Cell-based assay | Animal-based (LD50) assay | Animal-based (LD50) assay |
| Packaging (U/vial) | 50 or 100 | 300 or 500 | 50 or 100 | 100 | 50 and 100 |
| GL Units (U) b | 20 | 50 | 20 | 20 | 40 |
| Storage before reconstitution | 2°C–8°C | 2°C–8°C | Room temperature | 2°C–8°C | Room temperature |
| Pricing vs Ona-BoNTA | … | Less | Less | Less | More |
| Median duration | 3–4 mo for GL | Up to 4 mo | Up to 4 mo | Up to 4 mo | 6 mo |
a RTP004: 5-kDa proprietary stabilizing excipient peptide.
b Units are not interchangeable between each commercially available BoNTA.
In some formulations (Ona-BoNTA, Abo-BoNTA, and Pra-BoNTA), the core 150-kDa neurotoxin is electrostatically complexed with accessory proteins (APs) that are natively expressed in the bacterial cell. These APs contribute to the overall molecular weight of the active product (see Table 1 ). During reconstitution with bacteriostatic saline, pH changes result in the disruption of weak electrostatic connections between the core toxin and APs, leading to dissociation.
Immunogenicity
Although APs do not influence BoNTA durability or diffusion, they have been linked to the development of neutralizing antibodies against BoNTA [ ]. This mechanism is thought to drive the clinical phenomenon of BoNTA “nonresponders” or reduction in response or durability of BoNTA overtime [ ]. For patients experiencing a loss of response or durability to BoNTA, or for patients who plan to have serial injections for medical indications (eg, migraines), BoNTA formulations lacking associated proteins may prove beneficial. Inco-BoNTA and Daxi-BoNTA are the only 2 commercially available products that do not contain APs (see Table 1 ).
Excipients
BoNTA products also differ in their excipients, which are inactive components added to stabilize the active product. Human serum albumin (HSA) is a shared excipient of all BoNTA formulations with the important exception of Daxi-BoNTA, contributing to many of its attractive clinical attributes [ , ]. HAS prevents aggregation of BoNTA to itself and the glass vial, preserving activity. Other common excipients include sugars, surfactants, sodium chloride, and buffers (see Table 1 ).
Potency
During manufacturing, purification processes remove bacterial cell contaminants and are followed by a finishing method that produces the BoNTA into a powdered form (see Table 1 ). Each BoNTA product must be evaluated to quantify its potency, which does not necessarily correlate to quantity of toxin protein. BoNTA potency is expressed in units (U) and is defined as the biological activity of a given amount of nanogram (ng) toxin protein [ ]. BoNTA manufacturers each have unique assays to measure and quantify potency (U) and package their product (as U/vial) based on their specific assay [ ].
It is imperative to understand that no standardization exists for 1U of BoNTA, and units for each BoNTA formulation are noninterchangeable [ ]. For example, 1U of Abo-BoNTA is not the same as a 1U of Ona-BoNTA or Inco-BoNTA. To mitigate this lack of standardization, nanogram of active toxin protein per dose may be used to compare BoNTA formulations. However, this method is imprecise because quantity of protein product does not necessarily correlate to potency [ ].
Daxibotulinumtoxin A: unique formulation and clinical profile
RTP004
As mentioned, Daxi-BoNTA is the only available BoNTA without the stabilizing excipient, HAS [ , ]. Instead, RTP004, a novel proprietary 5-kDa synthetic peptide, acts as its stabilizing excipient. RT004 contains 35 amino acids with 15 consecutive lysine residues, which form strong electrostatic bonds with Daxi-BoNTA. Flanking these lysine residues is a 10 amino acid protein transduction domain (PTD). Engineered from the human immunodeficiency virus protein, PTD provides the excipient with cell-penetrating abilities, which have been used for intracellular molecular delivery in other pharmaceuticals [ ].
RTP004 prevents aggregation of toxin to glass vial and ensures sustained retention of toxin during manufacturing and transport [ , ]. Importantly, its synthetic derivation precludes RTP004 from exhibiting immunogenicity [ ].
Improved Efficacy and Durability
Following local injection, effective binding of BoNTA to the nerve terminal of the intended muscle is an intricate process. The small concentration of BoNTA must diffuse through the extracellular space to locate and selectively bind to the target nerve terminal. Negatively charged glycosphingolipids in the nerve terminal’s cellular membranes serve as binding sites for positively charged BoNTA residues [ ]. Binding of BoNTA to glycosphingolipids permits translocation of neurotoxin and contributes to durability and duration of action as BoNTA is held and accumulated at the nerve terminal [ ].
All BoNTAs contain positively charged amino acids that bind to glycosphingolipids. However, the RTP004 excipient of Daxi-BoNTA, with its positively charged lysine residues and flanking PTD, is postulated to facilitate and intensify its binding to glycosphingolipids [ ]. This is supported by findings from preclinical studies that BoNTA with RTP004 excipient had superior binding to nerve terminals compared with identical BoNTA without RTP004 [ ].
Increased binding of Daxi-BoNTA to the nerve terminal reduces loss of Daxi-BoNTA and potentiates the availability of BoNTA for endocytosis into the neuron. Furthermore, the accumulation of more product at the nerve terminal allows for continued endocytosis overtime, explaining its extended duration of action compared with other commercially available BoNTAs (see Table 1 ) [ ].
Superior Diffusion
Diffusion is defined as the ability of toxin to passively move along a concentration gradient within the target muscle. Diffusion is different from spread , defined as the inadvertent migration of toxin to unintended treatment areas, which may lead to adverse events such as ptosis.
BoNTA typically has the greatest clinical effect at the point of injection with tapering, subtle effects on the surrounding muscle fibers due to diffusion limitations. This may result in uneven muscle paralysis and a patchwork appearance of intervening retained rhytids within a treated area [ ]. This phenomenon is commonly experienced when treating the broad frontalis muscle, where injections are avoided in the inferior portion of the muscle to reduce risk of spread and brow ptosis [ ]. Although diffusion from superior frontalis injections is intended to treat the inferior portion of the frontalis, diffusion is occasionally suboptimal leading to compensatory recruitment and worsening of inferior frontalis lines above the brow.
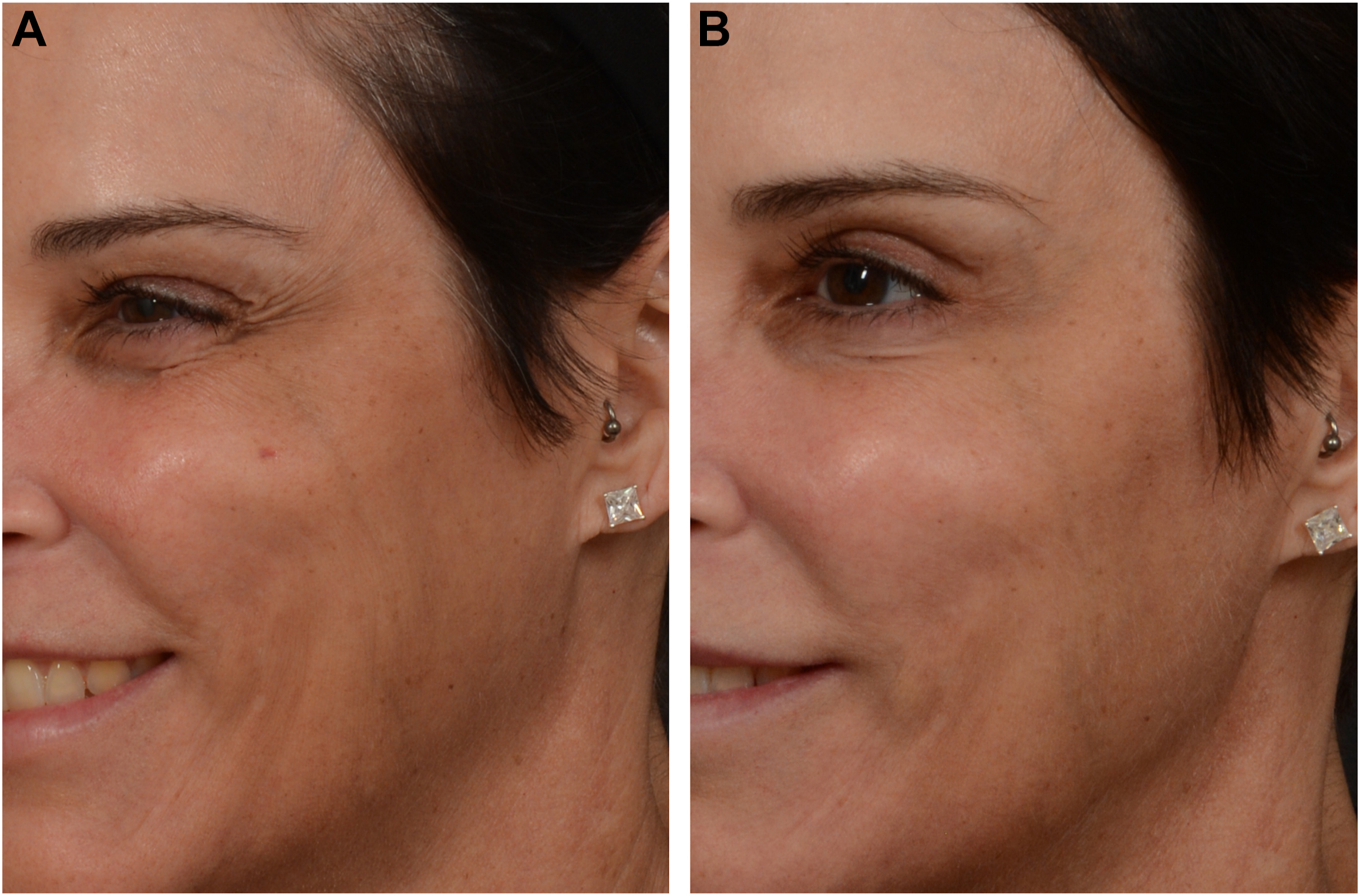
Anecdotally, Daxi-BoNTA seems to exhibit superior diffusion similar to that of Abo-BoNTA. This is attributed to RTP004’s ability to improve the binding and retention of Daxi-BoNTA at nerve terminals, facilitating its passive movement along the treated muscle and wider extension of clinical effect [ ]. Optimal diffusion contributes to the more even “field effect” clinically described, likely most beneficial when treating broad muscles such as the frontalis or orbicularis oculi [ ]. For example, optimal diffusion along the entire orbicularis oculi may explain the reduction in recruitment of compensatory medial muscle movements following Daxi-BoNTA treatment of lateral canthal lines (LCL; Fig. 1 A and B ). Superior diffusion may also contribute to the reduced need for “touch-ups” observed with Daxi-BoNTA.
Related posts:
 Festoon Evaluation and Management
Festoon Evaluation and Management
 Updates on Neuromodulators
Updates on Neuromodulators
 Nonsurgical Approach for Neck Rejuvenation
Nonsurgical Approach for Neck Rejuvenation
 Cannula Versus Needle for Rejuvenation of the Perioribital Region
Cannula Versus Needle for Rejuvenation of the Perioribital Region
 Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


