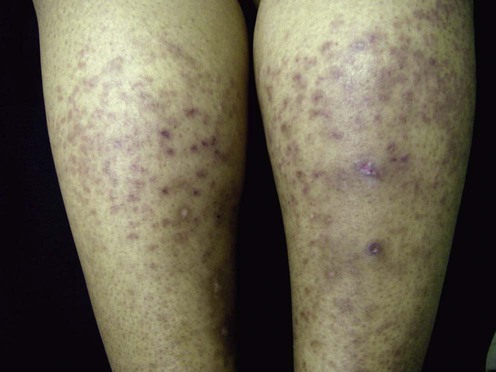
50 Cutaneous polyarteritis nodosa Cindy E. Owen and Jeffrey P. Callen Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Polyarteritis nodosa (PAN) is a necrotizing vasculitis that involves small or medium-sized arterioles. Classic PAN is characterized by fever, weight loss, cutaneous ulcers, livedo reticularis, myalgias and weakness, arthralgias or arthritis, neuropathy, abdominal pain, ischemic bowel, testicular pain, hypertension, and renal failure. Microscopic polyarteritis (MPA) involves the same-sized vessels as well as smaller vessels, and is manifest clinically as a glomerulonephritis and a pulmonary capillaritis with alveolar hemorrhage. Patients with MPA may develop small vessel vasculitis (palpable purpura), livedo reticularis with or without nodules, and/or ulcerations of the skin. Cutaneous PAN (cPAN), sometimes termed benign cutaneous polyarteritis, is characterized by livedo reticularis, nodules and ulceration, usually of the leg; it has been postulated to be a localized necrotizing arteritis that does not affect internal organs, and runs a chronic but benign course. Many reports, however, have linked cPAN to inflammatory bowel disease, streptococcal upper respiratory infection, or hepatitis B or C infection. Occasional reports have linked cPAN to antiphospholipid antibodies, cryoproteins, or antineutrophil cytoplasmic antibodies. One recent report has demonstrated that interleukin-6 is elevated in roughly 40% of patients (Kawakami, T., et al., 2012. Acta Derm Venereol 8;92 (3), 322–323). Some cases have occurred in patients treated with propylthiouracil and minocycline. cPAN appears to be more prevalent in children. Although it is generally benign, there have been reports of associated neuropathy, as well as visceral involvement. Management strategy cPAN causes pain and discomfort and may ulcerate, thereby causing disability. Therapy may include local measures, e.g., gradient pressure stockings, or systemic therapies, including systemic corticosteroids, methotrexate, azathioprine, pentoxifylline, and intravenous immuneglobulin (IVIG). Most of the reports are anecdotes or small case series. Specific investigations Skin biopsy Serology for hepatitis B and C, anti-streptolysin O antibody titers, antineutrophil cytoplasmic antibodies, antiphospholipid antibodies, and cryoproteins Assessment for systemic involvement Assessment for inflammatory bowel disease Assessment for drugs that have been linked to cPAN Cutaneous periarteritis nodosa: a clinicopathological study of 79 cases. Daoud MS, Hutton KP, Gibson LE. Br J Dermatol 1997; 136: 706–13. This retrospective analysis of 79 patients evaluated the clinical and histological features of cPAN and attempted to identify any clinical, pathological, and immunological differences that may distinguish those cases likely to have a prolonged course. During the course of their illness 39 patients had ulcers. Women were affected more than men. Painful nodules on the lower extremities, with edema and swelling, were the most common clinical finding; 22% of patients had some evidence of neuropathy. Most of the laboratory findings were non-specific. There was no evidence for hepatitis B infection in the 37 patients tested, and hepatitis C infection was present in only one of the 20 patients tested. Five patients had inflammatory bowel disease (four had Crohn disease and one had ulcerative colitis). Ten patients had rheumatoid arthritis. Most patients (60%) had no associated medical condition. The disease course was prolonged but benign, and systemic PAN did not develop in any patient. The ulcerative form of disease was more prolonged and frequently associated with neuropathy. Therapy was varied, and the patients with non-ulcerative disease responded better than those with ulcers. Observations suggested that agents such as corticosteroids, azathioprine, pentoxifylline, and hydroxychloroquine were effective in individual patients. This study highlights the associations that might occur in up to 40% of patients, the fact that neuropathy is relatively common, and that the course and response to treatment are dependent on the presence of ulceration. Only gold members can continue reading. Log In or Register to continue Related Related posts: Mucoceles Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Rocky Mountain spotted fever and other rickettsial infections Stay updated, free articles. Join our Telegram channel Join Tags: Treatment of Skin Disease Comprehensive Therapeutic Strategies Aug 7, 2016 | Posted by admin in Dermatology | Comments Off on Cutaneous polyarteritis nodosa Full access? Get Clinical Tree Get Clinical Tree app for offline access Get Clinical Tree app for offline access
50 Cutaneous polyarteritis nodosa Cindy E. Owen and Jeffrey P. Callen Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports Polyarteritis nodosa (PAN) is a necrotizing vasculitis that involves small or medium-sized arterioles. Classic PAN is characterized by fever, weight loss, cutaneous ulcers, livedo reticularis, myalgias and weakness, arthralgias or arthritis, neuropathy, abdominal pain, ischemic bowel, testicular pain, hypertension, and renal failure. Microscopic polyarteritis (MPA) involves the same-sized vessels as well as smaller vessels, and is manifest clinically as a glomerulonephritis and a pulmonary capillaritis with alveolar hemorrhage. Patients with MPA may develop small vessel vasculitis (palpable purpura), livedo reticularis with or without nodules, and/or ulcerations of the skin. Cutaneous PAN (cPAN), sometimes termed benign cutaneous polyarteritis, is characterized by livedo reticularis, nodules and ulceration, usually of the leg; it has been postulated to be a localized necrotizing arteritis that does not affect internal organs, and runs a chronic but benign course. Many reports, however, have linked cPAN to inflammatory bowel disease, streptococcal upper respiratory infection, or hepatitis B or C infection. Occasional reports have linked cPAN to antiphospholipid antibodies, cryoproteins, or antineutrophil cytoplasmic antibodies. One recent report has demonstrated that interleukin-6 is elevated in roughly 40% of patients (Kawakami, T., et al., 2012. Acta Derm Venereol 8;92 (3), 322–323). Some cases have occurred in patients treated with propylthiouracil and minocycline. cPAN appears to be more prevalent in children. Although it is generally benign, there have been reports of associated neuropathy, as well as visceral involvement. Management strategy cPAN causes pain and discomfort and may ulcerate, thereby causing disability. Therapy may include local measures, e.g., gradient pressure stockings, or systemic therapies, including systemic corticosteroids, methotrexate, azathioprine, pentoxifylline, and intravenous immuneglobulin (IVIG). Most of the reports are anecdotes or small case series. Specific investigations Skin biopsy Serology for hepatitis B and C, anti-streptolysin O antibody titers, antineutrophil cytoplasmic antibodies, antiphospholipid antibodies, and cryoproteins Assessment for systemic involvement Assessment for inflammatory bowel disease Assessment for drugs that have been linked to cPAN Cutaneous periarteritis nodosa: a clinicopathological study of 79 cases. Daoud MS, Hutton KP, Gibson LE. Br J Dermatol 1997; 136: 706–13. This retrospective analysis of 79 patients evaluated the clinical and histological features of cPAN and attempted to identify any clinical, pathological, and immunological differences that may distinguish those cases likely to have a prolonged course. During the course of their illness 39 patients had ulcers. Women were affected more than men. Painful nodules on the lower extremities, with edema and swelling, were the most common clinical finding; 22% of patients had some evidence of neuropathy. Most of the laboratory findings were non-specific. There was no evidence for hepatitis B infection in the 37 patients tested, and hepatitis C infection was present in only one of the 20 patients tested. Five patients had inflammatory bowel disease (four had Crohn disease and one had ulcerative colitis). Ten patients had rheumatoid arthritis. Most patients (60%) had no associated medical condition. The disease course was prolonged but benign, and systemic PAN did not develop in any patient. The ulcerative form of disease was more prolonged and frequently associated with neuropathy. Therapy was varied, and the patients with non-ulcerative disease responded better than those with ulcers. Observations suggested that agents such as corticosteroids, azathioprine, pentoxifylline, and hydroxychloroquine were effective in individual patients. This study highlights the associations that might occur in up to 40% of patients, the fact that neuropathy is relatively common, and that the course and response to treatment are dependent on the presence of ulceration. Only gold members can continue reading. Log In or Register to continue Related Related posts: Mucoceles Tinea capitis Herpes genitalis Necrolytic migratory erythema Nevoid basal cell carcinoma syndrome Rocky Mountain spotted fever and other rickettsial infections Stay updated, free articles. Join our Telegram channel Join Tags: Treatment of Skin Disease Comprehensive Therapeutic Strategies Aug 7, 2016 | Posted by admin in Dermatology | Comments Off on Cutaneous polyarteritis nodosa Full access? Get Clinical Tree