Cutaneous Manifestations of Internal Disease and Metastases
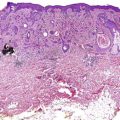
Figure 10-1(A) Trichodiscomas and (B) fibrofolliculomas and acrochordons in a patient with Birt-Hogg-Dubé.(With permission López V, Jordá E, Monteagudo C. Birt-Hogg-Dubé Syndrome: An Update. Actas Dermo-Sifiliográficas (English Edition) 2012;103(3):198–206)
Genetics
• Folliculin (FLCN) gene mutation (involved in mTOR pathway)
Associations/comments
• Fibrofolliculoma, trichodiscoma, perifollicular fibroma and acrochordons are identical lesions just viewed in different histologic planes
• Important associated findings:
• Pulmonary cysts (most common; up to 90%) lead to spontaneous pneumothorax (30%)
• Multiple renal carcinomas (15%, most commonly chromophobe renal carcinoma and oncocytoma)
• Medullary thyroid carcinoma
• +/− colon cancer (inconclusive association)
Cardio-facio-cutaneous syndrome (CFC)
Cutaneous findings
• Coarse facies (long and broad), generalized ichthyosis-like scaling, keratosis pilaris, CALMs, nevi, and sparse curly hair
Genetics
• AD; one of the RASopathies; mutations in BRAF (most common) and other MAPK pathway genes
Associations/comments
• A/w mental retardation, pulmonic stenosis, atrial septal defect, hypertrophic cardiomyopathy, and short stature
• All RASopathies (CFC, NF1, Noonan, Costello syndromes, and LEOPARD) affect RAS/MAPK pathway and have similar clinical presentations → often need genetic tests to distinguish
Carney complex (LAMB and NAME syndromes)
Cutaneous findings
• LAMB = Lentigines, Atrial (and cutaneous) Myxomas, Blue nevi (classically epithelioid blue nevi)
• NAME = Nevi, Atrial (and cutaneous) Myxomas, Ephelides
Genetics
• AD, mutations in PRKAR1A gene (encodes subunit of Protein Kinase A)
• Skin involvement in 60%; LCV, urticaria, livedo reticularis, subcutaneous nodules, PNGD (palisaded neutrophilic granulomatous dermatitis), and extravascular granulomas
Associations/comments
• Most commonly a/w allergic rhinitis, severe asthma, peripheral eosinophilia of ≥10%, sinusitis, transient pulmonary infiltrates, and mononeuritis multiplex
• ↑IgE levels
• Most common causes of mortality: myocarditis and coronary arteritis
• ANCAs detectable in 50%; p-ANCA (anti-MPO) ≫ c-ANCA (PR-3)
• ANCAs less frequently positive compared with Wegener’s (50% vs ~100%)
• May be a/w leukotriene inhibitors (montelukast and zafirlukast)
Costello syndrome
Cutaneous findings
• Lax skin on hands and feet, coarse facies, low-set ears, deep palmoplantar creases, periorificial papillomas, acanthosis nigricans, and curly hair
Genetics
• AD, one of the RASopathies; mutations in HRAS (85%) > KRAS (10%–15%)
Associations/comments
• A/w mental and growth retardation, pulmonic stenosis, hypertrophic cardiomyopathy, and arrhythmias
• ↑risk of rhabdomyosarcoma and transitional cell (bladder) CA
• All RASopathies (CFC, NF1, Noonan, Costello syndromes, and LEOPARD) have similar clinical presentations → need genetic tests to distinguish
Cutis laxa
Cutaneous findings
• Loose, pendulous skin of face (esp. periocular and cheeks→ “bloodhound facies”), neck, axillae, and thighs; skin lacks elastic recoil (vs EDS)
Genetics
• Multiple forms:
• AR: most common and most severe; Fibulin-5 (FBLN5)
• AD: benign course; Elastin (ELN) > FBLN5
• XLR: ATP7A (copper transporter)
Associations/comments
• Occipital horn syndrome is the current name for XLR cutis laxa, (which was also formerly called Ehlers-Danlos type IX); OHS a mild variant of Menkes kinky hair syndrome
• AR cutis laxa is most frequently a/w internal organ dysfunction and death:
• AD; caused by mutations in collagen III (COL3A1)
Associations/comments
• Most dangerous form of EDS because of the risk of death from rupture of internal organs (arterial rupture > GI tract [esp. sigmoid colon], uterus [particularly in pregnancy])
Hereditary hemorrhagic telangiectasia (pulmonary disease in type I > type II)
Cutaneous findings
• Multiple macular/“mat-like” telangiectasias most commonly on lips, oral mucosa, and extremities (Fig. 10-2)
Figure 10-2Patient with HHT and multiple telangiectasias on tongue and lip.(With permission Irani F, Kasmani R. Hereditary hemorrhagic telangiectasia: fatigue and dyspnea. Can Med Assoc J 2009;180(8):839–839)
Genetics
• AD, mutations in genes involved in TGF-β transduction pathway:
• HHT1 = endoglin (ENG)
• HHT2 = Alk-1 (ACVRL1)
Associations/comments
• Epistaxis (often the initial symptom), AV malformations of lungs (HHT-1 most commonly), liver (HHT-2 most commonly) and CNS; recurrent upper GI hemorrhage
• *Mnemonic: “Alk-1 is a/w liver” (think of Alkaline phosphatase, which is found in liver)
• AR; caused by a variety of mutations leading to ↑homocysteine levels in blood and urine; most common = cystathionine β-synthase (CBS gene)
• Other gene mutations: MTHFR, MTR, MTRR, and MMADHC
Associations/comments
• A/w atherosclerosis and vascular thrombosis (arterial + venous)
• A/w mental retardation and seizures
Hyperlipoproteinemias
Cutaneous findings
• Type I (familial LPL deficiency and hyperchylomicronemia): eruptive xanthomas
• Type II (familial hypercholesterolemia): tendinous, tuberous, tuboeruptive, interdigital xanthomas (pathognomonic), and plane xanthomas
• Type III (familial dysbetalipoproteinemia, “broad beta disease”): tendinous, tuberous, tuboeruptive xanthomas, and plane xanthomas of palmar creases (pathognomonic)
• Type IV (endogenous hypertriglyceridemia): eruptive xanthomas
• Type V: eruptive xanthomas
Genetics
• Type I: LPL deficiency and ApoC-II deficiency
• Type II: LDL receptor defect and ApoB-100 defect
• Type III: ApoE abnormality (results in ↓hepatic clearance)
• Type IV: ↑VLDL as a result of diabetes, alcoholism, and/or obesity
• Type V: ↑chylomicrons and VLDL; as a result of diabetes
Associations/comments
• Associated systemic findings:
• Type I, type IV, and type V: acute pancreatitis (as a result of ↑TGs)
• Type II and III: atherosclerosis → MI and stroke
• High fever lasting ≥5 days, cervical lymphadenopathy, truncal rash, hand edema/desquamation, oral findings, and conjunctival injection are diagnostic features
• Rx: high dose ASA and IVIG are essential to prevent coronary disease
LEOPARD syndrome
Cutaneous findings
• Lentigines (upper half of body; appear in childhood), CALMs, ocular hypertelorism (widely spaced eyes), low-set ears
Genetics
• AD; is one of the RASopathies; most common mutation is PTPN11 gene (90%)
• Less common mutations in MAPK pathway (10%): BRAF and RAF1
Associations/comments
• ECG abnormalities, Pulmonary stenosis, Abnormalities of genitalia (cryptorchidism #1, hypospadias), Retardation of growth, and Deafness
• Hard to clinically distinguish from other RASopathies (CFC, NF1, Noonan, and Costello syndromes)
Lymphomatoid granulomatosis
Cutaneous findings
• Dermal or SQ nodules +/− ulceration on trunk and extremities
• CALMs, axillary freckles (“Crowe’s sign”; seen in 30%; may involve neck and other intertriginous sites), multiple neurofibromas, and Lisch nodules (iris)
Genetics
• AD; mutation in NF1 gene (neurofibromin)
Associations/comments
• A/w HTN (essential HTN and 2° to pheochromocytoma)
Primary systemic amyloidosis (AL amyloidosis)
Cutaneous findings
• Petechiae/pinch purpura most common skin finding; may also see shiny, translucent waxy papulonodules or plaques, alopecia, and macroglossia
Associations/comments
• A/w restrictive cardiomyopathy, conduction abnormalities, and proteinuria
• As a result of deposition of immunoglobulin light chains (AL) in skin and internal tissues; deposits stain pink-red w/ Congo red (apple-green birefringence on polarized light)
• Primary systemic amyloidosis a/w skin findings in 30%; secondary systemic amyloidosis does NOT produce clinical skin changes
Progeria (Hutchinson-Gilford progeria)
Cutaneous findings
• Sclerodermoid changes, characteristic facies (prominent eyes, thin beaked nose, protruding ears, and micrognathia), mottled hyperpigmentation, ↓SQ fat, and alopecia
Genetics
• AD; mutations in lamin A (LMNA gene; component of nuclear lamina)
Associations/comments
• Most important association: premature death as a result of atherosclerosis, MI, or stroke
Psoriasis
Associations/comments
• ↑risk of cardiovascular, cerebrovascular, and peripheral arterial diseases; ↑risk of metabolic syndrome
Relapsing polychondritis
Cutaneous findings
• Intense erythema of cartilaginous portion of ears (spares earlobes) + inflammation of other cartilaginous tissues (nose and trachea)
Associations/comments
• A/w tracheal and nasal collapse
• A/w aortic insufficiency and dissecting aortic aneurysm
Rheumatic fever
Cutaneous findings
• Erythema marginatum, subcutaneous nodules, polyarthritis, chorea, and fever
Associations/comments
• Acute phase: pericarditis
• Chronic: mitral and aortic valve disease
Sarcoidosis
Cutaneous findings
• Red-brown papules, nodules, and plaques w/ “apple jelly” color on diascopy; may arise in preexisting scars; lupus pernio (strongly a/w lung disease), EN (a/w acute bilateral hilar adenopathy and arthritis of ankles = Lofgren syndrome)
Associations/comments
• Pulmonary: pulmonary artery HTN and interstitial lung disease
• Severe (>90% mortality if untreated) multisystem necrotizing vasculitis
• Most common systemic manifestations: respiratory tract (chronic sinusitis is most common presenting symptom of GPA); renal (segmental crescentic necrotizing glomerulonephritis)
• c-ANCA (anti-Proteinase-3) autoantibodies in ~100% of pts by ELISA and IIF; detectable ANCAs more common in GPA than in Churg-Strauss (50%)
Yellow nail syndrome
Cutaneous findings
• Thick, slow-growing, highly curved, and yellow or yellow-green nails w/ onycholysis; absent cuticles and lunulae
Associations/comments
• Classic triad: yellow nails, lymphedema, and pulmonary disease (bronchiectasis and pleural effusions)
• Velvety, brown, digitate plaques on neck and in axillary and inguinal folds
Associations/comments
• Slow onset, usually manifests earlier in life
• Can indicate insulin resistance and/or diabetes
• More common in darkly pigmented individuals
• Treatment includes improvement of insulin resistance, topical retinoids, ammonium lactate, and calcipotriene
Granuloma annulare
Cutaneous findings
• Often affects trunks and extensor limbs, or may be generalized and eruptive; p/w nonscaly, flesh-colored, pink, violaceous, or reddish brown papules that can be grouped in an arcuate or annular pattern
Associations/comments
• Usually asymptomatic and spontaneously resolves over months to years