■ Motor innervation (Tables 8-3, 8-4 and Fig. 8-5)
○ Muscles of facial expression are innervated by CN VII (facial nerve); facial muscles receive motor innervation from their underside
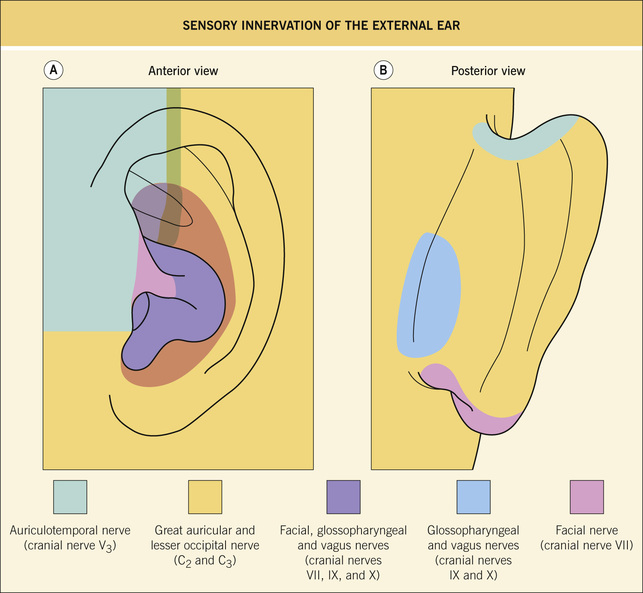
♦ Boards Factoid: as a minor function, CN VII also provides sensory input for anterior tongue (via chorda tympani branch) and a small amount of the external auditory meatus
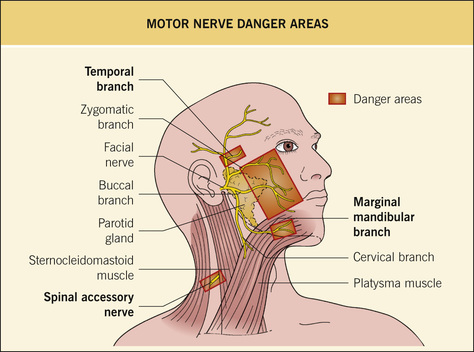
○ Facial nerve emerges from the stylomastoid foramen; the nerve travels within the parotid gland and then splits into 5 branches: temporal, zygomatic, buccal, mandibular, and cervical branches (“To Zanzibar By Motor Car”)
Table 8-3
Motor Innervation of the Head and Neck
Table 8-4
Cutaneous Danger Zones
| Target Structure | Danger Zone | Associated Adverse Event | Other Comments |
| Vascular occlusion from filler/steroid injections | |||
| Labial/angular artery | Near base of ala | Skin necrosis | Rx: nitroglycerin paste, LMWH, and hyaluronidase (if HA filler) |
| Supratrochlear artery | Glabellar region | Skin necrosis, blindness | Same as above |
| Motor nerve injury | |||
| Temporal nerve | Most susceptible to injury as it crosses over the zygomatic arch | Unilateral frontalis paralysis, eyelid ptosis | Temporal nerve runs a diagonal course from 0.5 cm below the tragus to 1.5 cm above the lateral brow; nerve is superficially located within the facia as it crosses the zygomatic arch |
| Zygomatic nerve (less common) | Malar cheek | Inability to completely close eyes ➔ corneal desiccation | Main trunks of zygomatic and buccal branches of facial nerve lie fairly deep ➔ less commonly injured than temportal and marginal mandibular |
| Marginal mandibular nerve | Most susceptible 2–3 cm inferolateral to oral commissure, as it passes over the mandible | Facial asymmetry upon smiling (normal at rest), and inability to protrude lower lip, drooling | |
| Spinal accessory nerve (cranial nerve XI) | Most susceptible to injury at Erb’s point = site where cervical plexus emerges; located along posterior border of SCM) | Winged scapula, inability to abduct arm, and shoulder pain | Erb’s point localization: 6 cm inferior to the midpoint of an imaginary line drawn between the mastoid process and angle of jaw Great auricular and lesser occipital nerves also arise from Erb’s point |
| Ulnar nerve | Susceptible to injury around medial epicondyle of humerus | “Claw-hand” deformity; weakness in wrist flexion, loss of flexion of fourth and fifth digits, and loss of sensation in ulnar distribution | — |
| Other | |||
| Parotid duct | A line drawn from tragus to mid portion of the upper lip approximates its course; duct courses over masseter, pierces buccinator, and drains into the mouth at second upper molar | Parotid duct injury ➔ sialocele (distinguished from a seroma by ↑↑amylase levels) | Rx: repair via microsurgery |
8.2 Surgical instruments and needles
■ Bard-Parker standard handle (most common): flat; holds common blades such as the #15, #11, and #10
■ Beaver handle: round or hexagonal; holds smaller, sharper blades; useful for confined spaces or delicate tissue
○ Short-handled scissors useful for delicate work
○ Long-handled scissors extend the surgeons reach and are useful for undermining
○ Curved blades useful for undermining cysts
○ Straight blades useful for trimming tissue and cutting sutures
○ Serrated blades grab tissue better
○ Sharp-tipped scissors puncture tissue easily and are best for dissection
○ Blunt-tipped scissors are best for delicate undermining
○ Iris scissors: sharp-tipped and short-handled; blades may be straight or curved; best for sharp dissection
○ Gradle scissors: similar to iris but blades curved and tapered to a fine point at tip; best for dissection of delicate tissue such as periorbital skin
○ Westcott scissors: spring-loaded instrument similar in appearance to Castro-Viejo; good for delicate eyelid dissection
○ Mayo scissors: characterized by its ~1 : 1 handle-to-blade ratio; primary purpose is coarse dissection
○ Metzenbaum scissor: long handles with blunt tips ➔ useful for blunt dissection in areas that require long reach
○ Supercut scissors: one blade has a razor edge; “supercut” blades are available on most scissor types listed above and often are denoted with black handles
○ Smaller needle drivers with smooth jaws
♦ Ideal for small, delicate needles
♦ Advantages: smooth jaws have ↓risk of tearing small sutures (6-0 and smaller) and are less damaging to fine needles (P-3 and smaller)
♦ Disadvantages: needles not grasped as tightly as with serrated needle drivers ➔ ↑needle twisting
♦ Caution: larger needles will ruin small needle drivers
♦ Ideal for larger needles and work on trunk
♦ Advantages: serrated jaws hold needles more securely (prevents twisting)
♦ Disadvantage: damages delicate needles, shreds small sutures
○ Serrated forceps: easier to grab needle, but results in ↑tissue crush injury
○ Toothed forceps: harder to grasp needle, but handles tissue gently (↓crush injury)
○ Combination forceps: have both teeth as well as serrated platforms ➔ allows for gentle tissue handling and easier grasping of needle
○ Adson: relatively large forceps; useful for trunk and extremities
○ Bishop-Harmon forceps: small, fine-tipped instruments; most useful for delicate tissues such as the eyelids; always have 3 holes in handles to make them lighter in weight and easier to grip
○ Jeweler’s forceps: have very pointy ends; most useful for suture removal
■ Hemostats: used to grasp bleeding vessels before ligation
■ Skin hooks: available in many forms;
○ “Skin rake”: a skin hook with multiple hooks
○ Hooks are the least traumatic way to handle tissue (during electrosurgery and suturing), but are a sharps hazard
■ Periosteal elevator: used to remove periosteum or separate nail plate from nail bed
■ Chalazion clamp: useful for eyelid surgery or on the lip to stop bleeding needles
■ Needle is composed of three parts:
○ Shank (swage): swaged portion that attaches to suture; weakest part of needle ➔ do NOT grasp here, it will bend or break the needle
♦ Size of suture track is determined by shank size, not suture size
○ Body: middle part; strongest portion of needle ➔ always grasp here with needle driver; comes in various curvatures (most common is 3/8 circle)
○ Tip: sharp tip that may be round (tapered) or cutting; minimize grasping of tip ➔ contact w/ other instruments quickly dulls the tip
○ Round (tapered): only the tip pierces tissue (no sharp edges along arc of needle); is less likely than cutting needles to tear tissues; used for deep soft tissues (fat and muscle); difficult to pass through skin
○ Cutting: triangular-shaped needle point; preferred for skin because it easily passes through tissue; two types:
♦ Conventional cutting: cutting surface is on inner portion of needle arc; ↑risk of sutures tearing through wound edge (this is because the cutting edge of needle faces toward the wound edge)
♦ Reverse cutting: cutting surface is on outer portion of needle arc; ↓risk of sutures tearing through wound edge
For a more detailed discussion on surgical tools, please read: Weber LA. The surgical tray. Dermatol Clin. 1998 Jan;16(1):17–24. PMID: 9460575.
8.3 Suture techniques
■ Surgeon’s knot: most commonly used; essentially a square knot; first knot is double thrown to prevent slippage
■ Aberdeen hitch knot: used to tie the end of a running subcutaneous suture; is more compact, more secure, and uses less material than surgeon’s knot
• Cuticular/epidermal suturing
■ Simple interrupted: used for wounds under moderate to high tension; directing the needle away from the wound results in ↑eversion and less frequent sunken scars
■ Simple running: used for wounds under minimal tension; faster to place than interrupted sutures; ↑risk of wound dehiscence
■ Running locked sutures: provides hemostasis, but has risk of strangulation
■ Vertical mattress: strongly everts (Vertical = eVert) wound edges, eliminates dead space, and decreases wound edge tension
■ Horizontal mattress: provides hemostasis (Horizontal = Hemostasis), eliminates dead space, and decreases wound edge tension; significant strangulation risk ➔ do not use in poorly vascularized areas
■ Pulley suture: modified vertical mattress suture; used for wounds under high tension
■ Running horizontal mattress: same benefits as simple horizontal mattress, but is faster, provides ↑eversion, and ↓strangulation risk; improved outcomes relative to simple running sutures, but takes longer
■ Tip stitch: best stitch for flap and M-plasty tips; is a half-buried horizontal mattress suture
■ High-low (step-off stitch): used to correct imprecise dermal/subcuticular suturing, where one side of the wound edge is higher than the other (“step-off”)
• Subcuticular/dermal suturing
■ Simple buried suture: traditional intradermal suture; results in minimal wound eversion and high rate of spitting sutures
■ Buried vertical mattress: has one exit point in the subcutaneous plane; everts tissue more than a simple buried suture
■ Set-back suture (“buried butterfly”): suture entry and exit points are both underneath the undermined wound surface; everts tissue maximally; results in ↓spitting sutures and ↑cosmetic outcomes than the buried vertical mattress technique
■ Running subcuticular: running sutures in superficial dermis, instead of along epidermal surface; primary advantage = lack of track marks; however, ↑rate of spitting sutures; typically used in combination w/ buried vertical mattress sutures
■ Purse-string: traditionally used to ↓wound size and ↓healing time, relative to second intention; a recent RCT study did not demonstrate any difference in cosmetic appearance or scar size, but there was a trend toward faster healing time
■ Pulley suture: buried (subcuticular) pulley suture is essentially just a series of two or more simple buried subcuticular sutures; primary advantage = permits wound closure under high tension; disadvantage = tissue strangulation
■ “Figure of 8”: main suturing method used to tie off bleeding vessels
• Suture removal recommendations (largely anecdotal): head/neck ≤7 days, extremities/torso = 10 to 14 days; the longer the sutures remain in place ➔ ↓likelihood of dehiscence, but ↑cutaneous track-marks
• Suspension sutures: anchor the overlying tissue to periosteum ➔ removes tension from leading edge of flaps; prevents distortion of a free margin (especially eyelid), also prevents flap “tenting” across a concavity
8.4 Wound closure materials
• Suture types and properties (Tables 8-5 through 8-9)
Table 8-5
Suture Types
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


