Although some drugs cause only one clinical pattern of reaction, most are capable of producing several different types of reaction. 4 While most of these adverse reactions involve the skin, other organs such as the lungs, kidneys, liver, and lymph nodes may be affected singly or in various combinations.5. and 6. Since the teratogenic effects of thalidomide received widespread coverage approximately 50 years ago, this potential complication receives considerable experimental attention in the early testing of new compounds.7. and 8. Drug fever is another clinical manifestation of an adverse drug reaction.
Continuing advances in pharmacology have resulted in the introduction of an ever increasing number of drugs for therapeutic purposes with a consequent avalanche of case reports detailing adverse reactions.9. and 10. The true prevalence of cutaneous drug reactions is difficult to determine as most studies have been based on hospital inpatients, many of whom are receiving several drugs simultaneously.1. and 11. In these inpatient series, drug reactions have occurred in approximately 2% of patients; 12 this figure is probably not relevant to outpatients. The incidence has been lower in more recent studies. 13 About 2% of all drug reactions are considered life-threatening. 13 If looked at in another way, drug reactions are relatively uncommon when the number of reactions per course of drug therapy is considered. 12 Another important facet is the drug interaction in which one drug affects the action of another, usually by causing increased or decreased plasma levels of that drug. This so-called ‘pharmacokinetic reaction’ usually results from the influence of one or more of the drugs on the cytochrome P-450 isoenzyme system in the liver.14.15. and 16. Unlike adverse drug reactions, which are unpredictable in any specific patient, drug interactions are mostly known, and can be avoided. 17 Excellent reviews of the clinically significant drug interactions encountered in dermatology appeared in 200617 and 2008. 18
Diagnosing drug reactions
Attribution of a cutaneous reaction to a particular drug may be difficult since many patients receive many drugs simultaneously. 12 Furthermore, many drug reactions mimic various dermatoses, most of which may have other causes. Certain patterns are, however, frequently caused by drugs: these include exanthematous reactions, urticaria, photosensitive eruptions, fixed drug eruptions, erythema multiforme, and toxic epidermal necrolysis.1.4. and 19. Other factors that may be used to identify the offending drug include cessation of the suspected drug (dechallenge), rechallenge with the suspected drug at a later time (provocation), 20 the use of specifically designed computer algorithms, 21 a knowledge of drug reaction rates, and the morphology of lesions produced by particular drugs.9. and 22. Case reports, manufacturers’ brochures, and reporting systems have all contributed to our knowledge of the various reactions produced by particular drugs.22.23. and 24. A valuable monograph, updated regularly, is the Drug Eruption Reference Manual, produced by Jerome Z. Litt. Another important factor in identifying an offending drug is the timing of events. 23 Most drug reactions occur within 10 days of receiving the offending agent, although longer periods have been recorded. Furthermore, some drug reactions may persist for weeks to months after use of the drug has ceased. This applies particularly to reactions to gold. 19
Provocation tests, whereby the patient is challenged with the drug suspected of causing the reaction, may provide confirmation in over 50% of cases. 20 However, false-positive and false-negative reactions may occur, and there are also ethical considerations because in certain circumstances rechallenge may produce a severe anaphylaxis. 25 Some institutions are loath to give ethical approval for such procedures, although rechallenge is still being used to confirm the association in some countries. 26 Withdrawal tests are time-consuming if multiple drugs are involved. 10
The shortcomings of in-vivo testing and clinical observations have led to many studies being carried out to assess the reliability of various in-vitro tests. 10 Most have involved immunological methods as drug allergy is one mechanism involved in the pathogenesis of drug reactions. Some, such as skin testing, radioallergosorbent tests (RAST), and lymphocyte transformation studies, have been of limited diagnostic value. 26 Patch testing is usually of value only in allergic contact reactions, although positive patch tests have been found in up to 15% of patients with presumed drug reactions. 27 Positive reactions are more common with drugs such as β-lactams, clindamycin, and trimethoprim. 26 Prick and intradermal skin tests have also been used in the evaluation of drug reactions. 28
Drug-specific T cells may produce the inflammatory skin reaction through the production and release of different cytokines. Accordingly, T-cell-mediated sensitization to drugs may be assessed by assays based on cytokine release from peripheral blood lymphocytes. 29 One of the first tests used involved macrophage migratory inhibitory factor, but interferon gamma release29 and interleukin (IL)-5 detection can be used. One of the most sensitive tests appears to be that for macrophage migration inhibition factor (MIF), a lymphokine which is released when sensitized T lymphocytes are challenged with the appropriate antigen.9.10. and 30. It is seen with cell-mediated and some immediate-type reactions. 10 A positive MIF response to a variety of drugs has been found in 50–70% of patients with suspected drug eruptions but only in 5% of controls. 10 Interferon gamma release does not seem to be as accurate. 29 Tests based on the detection of drug-specific T-cell cytokines are a useful adjunct to clinical observations in detecting the offending drug.
Mechanisms of drug reactions
Various mechanisms, including toxic, metabolic, and allergic, have been implicated in the pathogenesis of cutaneous drug reactions. 31 Certain patient groups are at an increased risk of developing an adverse drug reaction, including women, patients with Sjögren’s syndrome, and those with the acquired immunodeficiency syndrome.13.32.33. and 34. It has been suggested that ‘pharmacogenetic variability’ may account for a susceptibility to certain serious drug reactions. 32 Examples include glutathione synthetase deficiency (particularly in patients with AIDS) predisposing to sulfonamide reactions, epoxide hydrolase deficiency leading to the anticonvulsant hypersensitivity syndrome (see p. 515), and defects in drug acetylation resulting in isoniazid reactions. 32 Most adverse effects, so-called type A reactions, are due to the pharmacological action of a drug. 35 A ‘toxic’ hypothesis does not explain all the characteristics of drug reactions. 36 For many substances the mechanism is still uncertain. The term ‘idiosyncratic drug reaction’ has been used for unpredictable reactions that occur in only a small percentage of patients receiving the drug and which do not involve known pharmacological properties of the drug. 37 This term includes many of the reactions thought to have an immunological basis (see below). Such reactions are called type B reactions.
Immunological (allergic) mechanisms are thought to account for less than 20% of all cutaneous drug reactions despite the fact that positive tests for MIF (see above) are found in over 50% of suspected cases.5. and 10. This is because secondary immunological events may develop in the course of some drug reactions which basically are not of immunological pathogenesis. 9
Immunological drug reactions have certain features that distinguish them from non-immunological reactions, although none is absolute. 38 They occur in only a small percentage of the population at risk; they may occur below the therapeutic range of the drug; and they appear after a latent period of several days, although this duration may be shorter on rechallenge. 38 Certain clinical patterns of drug reaction, such as systemic anaphylaxis, serum sickness, allergic and photoallergic contact dermatitis, fixed drug eruption, vasculitis, and the systemic lupus erythematosus-like syndrome, are characteristic of the immunological types of drug reaction.5.19.38. and 39. Urticaria may result from both immunological and non-immunological reactions, and some exanthematous reactions may have an immunological basis. The majority of allergic drug reactions are caused by antibiotics, blood products, anti-inflammatory agents, and inhaled mucolytics. 11
All four Gell and Coombs reactions may be involved in allergic reactions to drugs although cutaneous reactions have not been clearly shown to be cytotoxic (type II reaction) in nature.5. and 39. The most significant drug reactions involve immediate hypersensitivity (type I reaction) and are IgE mediated. 31 The best studied of this class of reaction is penicillin allergy, in which IgE antibodies to penicillin have been detected in the serum of affected individuals. Clinical manifestations of type I reactions include anaphylaxis, urticaria, and angioedema. Immune complexes (type III reaction) are involved in the pathogenesis of vasculitis, serum sickness, some urticarial and exanthematous reactions, systemic lupus erythematosus-like drug reactions, and possibly erythema multiforme and erythema nodosum, when due to drugs.31. and 39. Immunohistochemical analysis has identified CD8-positive T cells as the predominant epidermal T-cell subset in drug-induced maculopapular and bullous eruptions. 30 However, more recent studies have isolated a heterogeneous population of CD4+ lymphocytes which are drug specific.40. and 41. The cells, when stimulated, produce interleukin-5. This cytokine may be responsible for the tissue eosinophilia often seen in drug reactions. 40 It seems that CD8+ cells are not the predominant cell type, as once thought. CD1a+ dendritic cells have been found in the dermis in eruptions caused by some antibiotics. 42 Apart from exanthematous (morbilliform) drug reactions, delayed hypersensitivity (type IV reaction) is uncommonly the cause of drug reactions resulting from ingestion of a drug, although it is the usual mechanism involved following the topical application of a sensitizing drug. 31 Type IV reactions may also be involved in fixed drug eruptions and in certain mixed reactions, as occur in erythema multiforme. The role of the type IV reactions has expanded since the recognition of subtypes of delayed hypersensitivity, an acknowledgement of the heterogeneity of T-cell function. 35 Pichler has written an excellent paper on this subject. 35 Type IVa corresponds to Th1 reactions, type IVb to the Th2 reactions, type IVc to cytotoxic reactions mediated by perforin and granzyme B, and type IVd reactions with IL-8 production, resulting in neutrophil recruitment and activation, resulting in pustular exanthema. 35 Some type IVc (cytotoxic) functions are present in all type IV reactions (Table 20.1).
Exanthematous reactions, eczema, bullous and pustular exanthema
Type IVd
T cells (IL-8)
Pustular exanthema
The offending drug, or a metabolite of it, acts as a hapten that combines with tissue or plasma protein to form a complete antigen, which in turn stimulates some part of the immune system. 19 If the drug is of high molecular weight, it may be antigenic in itself. The method of administration of the drug and even environmental factors, such as an underlying infection or the presence of light of a suitable wavelength, may all influence the outcome. 19 The integrity of the cutaneous nerves in a particular area also influences the distribution and expression of drug reactions. In patients with leprosy the affected site is often spared in a drug reaction. 43 Unilateral involvement has been reported in a drug reaction to phenytoin in a patient with hemiplegia, 43 again emphasizing the importance of an intact nervous system in some drug reactions.
Much less is known about the non-immunological mechanisms involved in drug reactions. These may involve activation of effector pathways (such as opiates releasing mast cell mediators and non-steroidal anti-inflammatory drugs altering arachidonic acid metabolism), overdosage (as seen with hemorrhage produced by an excess of anticoagulants), metabolic alterations (isotretinoin affecting lipid metabolism and certain drugs affecting porphyrin metabolism), and cumulative toxicity (as seen with color changes resulting from the deposition of drug metabolites in the skin). 19 Drugs may also exacerbate a pre-existing dermatological condition. 19
CLINICOPATHOLOGICAL REACTIONS
Even though the skin can react in only a limited number of ways, there are still a bewildering number of clinicopathological presentations of drug reactions.23. and 44. Usually, several drugs can produce any particular reaction, although certain drugs are more likely than others to give a particular pattern. The characteristics of the drug that determine which reaction is produced are largely unknown in the case of allergic drug reactions.
Although the important modifications of each of the major tissue reaction patterns induced by drugs are discussed in the respective chapters of this book, there are important clues common to a number of reaction patterns. They are shown in Table 20.2. A pattern analysis of the histological features of drug-induced skin diseases was published in 2008. 45 The various entities are considered elsewhere in this book.
The most common reactions produced by drugs are exanthematous in type, followed by urticaria and angioedema. 1 Fixed drug eruptions have been the third most common pattern in some series, although they have been much less frequent in others. 1 The most severe drug reactions are exfoliative dermatitis, the Stevens–Johnson syndrome, and toxic epidermal necrolysis. Sometimes, the clinical features of a drug reaction are difficult to characterize into one of the named patterns. Many of these are maculopapular in nature. They are often included in the exanthematous reaction, even though they do not strictly resemble a viral exanthem. Included in this group is the maculopapular eruption that may develop in the course of the treatment of leukemia, corresponding to the stage of peripheral lymphocyte recovery. 46
The various reactions produced by drugs have been discussed in other chapters with the exception of the exanthematous reactions, the vegetative lesions produced by halogens, and the drug hypersensitivity syndrome. These reactions will be discussed in detail below, followed by a brief summary of the other cutaneous patterns produced by drugs.
EXANTHEMATOUS DRUG REACTIONS
Exanthematous eruptions (also described as morbilliform and as erythematous maculopapular eruptions) are the most common type of drug reaction, accounting for approximately 40% of all reactions.1. and 47. The rash develops 1 day to 3 weeks after the offending drug is first given, although the timing depends on previous sensitization. 23 Uncommonly, the onset is much later in the course of the drug therapy and rarely it may develop after administration of the drug has ended.
There are erythematous macules and papules that resemble a viral exanthem. Lesions usually appear first on the trunk or in areas of pressure or trauma. 19 They spread to involve the extremities, usually in a symmetrical fashion. A recent publication has drawn attention to a distinct pattern of involvement of the upper arms in exanthematous drug eruptions. 48 Such eruptions involve the T1 dermatome with a sharp linear margin of demarcation from the spared skin served by the C5 spinal nerves. In short, there is medial involvement and lateral sparing. This so-called ‘drug line’ corresponds to the dorsoventral pigmentary demarcation line seen in about 20% of individuals with black skin, but normally invisible in white skin and known as the Voigt–Futcher line. 48 Pruritus and fever are sometimes present. The eruption usually lasts for 1–2 weeks and clears with cessation of the drug. 19
Exanthematous eruptions occur in 50–80% of patients who are given ampicillin while suffering from infectious mononucleosis, cytomegalovirus infection, or chronic lymphatic leukemia or who are also taking allopurinol. 31 Amoxicillin and salazosulfapyridine may sometimes produce a similar reaction in the same circumstances.49.50. and 51. An exanthematous eruption also occurs commonly in patients with AIDS who are given co-trimoxazole (trimethoprim-sulfamethoxazole).2. and 52. It appears that patients with lymphotrophic viral infections are at increased risk for cutaneous drug reactions. 53 Other drugs which cause an exanthematous reaction include penicillin, erythromycin, streptomycin, tetracyclines, bleomycin, amphotericin B, sulfonamides, oral hypoglycemic agents, thiazide diuretics, barbiturates, chloral hydrate, benzodiazepines, phenothiazines, ticlopidine, 54 codeine, 55 buserelin acetate, 56 allopurinol, thiouracil, quinine, quinidine, gold, captopril, and the non-steroidal anti-inflammatory drugs.23. and 57.Ginkgo biloba has also produced a diffuse morbilliform eruption. 58 Codeine and pseudoephedrine have produced an eruption resembling scarlet fever. 59
The mechanisms involved in exanthematous reactions are now much clearer. There is a superficial, mainly perivascular lymphocytic infiltrate with a few eosinophils. CD4+ cells are mainly located in the perivascular dermis while both CD4+ and CD8+ cells are found at the dermoepidermal junction in equal number. 35 The infiltrating T cells are very active expressing many cytokines. Cytotoxic-T cells (more CD4 cells than CD8 cells) cause interface changes (cell death and vacuolar change) by a perforin-dependent and granzyme B-dependent killing mechanism. 35 Enhanced production of IL-5 by drug-specific T cells is common in different forms of drug allergies, including exanthematous reactions. This cytokine is a key factor in the maturation and activation of eosinophils. 35 Exanthematous reactions are largely of type IVc.
Histopathology
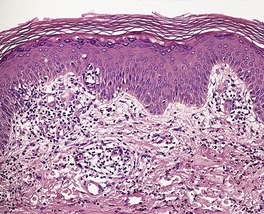
At first glance, the histological changes in the exanthematous drug reactions appear non-specific, but they are in fact quite characteristic. There are small foci of spongiosis and vacuolar change involving the basal layer with mild spongiosis extending one or two cells above this (Fig. 20.1). 60 A few lymphocytes are usually present in these foci. 60 A characteristic feature is the presence of rare apoptotic keratinocytes (Civatte bodies) in the basal layer (Fig. 20.2). Very focal parakeratosis may be present in lesions of some duration.
Fig. 20.1
Exanthematous drug reaction characterized by focal basal spongiosis, mild exocytosis of lymphocytes, and a perivascular infiltrate of lymphocytes in the upper dermis. (H & E)
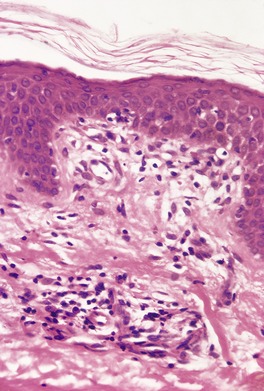
Fig. 20.2
Exanthematous drug reaction. A Civatte body (apoptotic keratinocyte) and a few lymphocytes are present in the basal layer. (H & E)
The papillary dermis is usually mildly edematous and there may be vascular dilatation. The inflammatory cell infiltrate, which consists of lymphocytes (some with large nuclei suggesting activation), macrophages, mast cells, occasional eosinophils and, rarely, a few plasma cells, is usually mild and localized around the superficial vascular plexus. 60
Epidermal changes may be minimal or even absent in scarlatiniform eruptions and in some non-specific maculopapular eruptions categorized as exanthematous for convenience.
HALOGENODERMAS
The term ‘halogenoderma’ includes iododerma, bromoderma,61. and 62. and the rare fluoroderma which result from the ingestion of iodides, bromides, and fluorides, respectively. 63 Iododerma is an uncommon disorder, while the other two are now exceedingly rare. 64 Verrucous plaques resembling those seen in the halogenodermas have recently been reported in two patients receiving long-term lithium therapy. 65
Three distinct types of cutaneous adverse reactions to bromides are seen: (i) acneiform papules, which may occur suddenly on the face, but which may spread over the neck, chest and arms; (ii) granulomatous lesions, known as bromoderma tuberosum; 66 and (iii) vegetative lesions.67. and 68.
The usual source of the iodide is the potassium salt used in expectorants and some tonics. 69 Rarely, radiocontrast media63. and 70. and amiodarone71 have been implicated. It may be due to systemic absorption from topical iodine, such as the use of a sitz bath containing povidone-iodine. 72 The characteristic lesion is a papulopustule which progresses to a vegetating nodular lesion. This may be crusted and ulcerated. There are usually a number of lesions, 0.5–2 cm in diameter, on the face, neck, back, or upper extremities.63.69. and 73. The lesions clear with cessation of the halide. The mechanism involved in their pathogenesis is uncertain. 63
In addition to vegetating lesions, iodides may also produce erythematous papules, urticaria, vesicles, carbuncular lesions, erythema multiforme, vasculitis, polyarteritis nodosa, and erythema nodosum-like lesions. 74 Iodides may also aggravate dermatitis herpetiformis, pyoderma gangrenosum, pustular psoriasis, erythema nodosum, and blastomycosis-like pyoderma.74. and 75.
The vegetating lesions show pseudoepitheliomatous hyperplasia with intraepidermal and some dermal abscesses.76. and 77. The abscesses contain a few eosinophils and desquamated epithelial cells in addition to the neutrophils. There may be occasional multinucleate cells in the dermis, but this is never the prominent feature that it is in chromomycosis and sporotrichosis, which the reaction superficially resembles. In early lesions the ‘intraepidermal’ abscesses can be seen to be related to follicular infundibula.
DRUG HYPERSENSITIVITY SYNDROME
A hypersensitivity reaction, characterized by fever, a generalized exanthem, and multiorgan toxicity, has been reported following the ingestion of a number of drugs including phenytoin sodium and other anticonvulsants (see p. 519), carbamazepine, sulfonamides, dapsone, calcium channel blockers, nevirapine, allopurinol, and piroxicam.78.79.80.81.82.83.84. and 85. Allopurinol is the major cause of this syndrome in Taiwan. 86 Recent reports have also incriminated bellamine, used for menopausal symptoms, 87 teicoplanin used with vancomycin, 88 vancomycin alone, 89 abacavir, 90 clomipramine, a tricyclic antidepressant, 91 efalizumab, 92 terbinafine, 93 and clopidogrel. 94 It is also known as the DRESS syndrome (drug rash with eosinophilia and systemic symptoms). 95 It is an idiosyncratic reaction which is fortunately rare. It may be fatal. It may occur after prolonged use of the drug, but many cases occur within 1–8 weeks after the intake of an anticonvulsant.96. and 97. The exact pathogenesis is unknown. Some patients have a genetic deficiency of epoxide hydrolase, a hepatic enzyme that detoxifies the arene oxide metabolites of antiepileptic drugs. 87 Infection with human herpesvirus-6 (HHV-6) and possibly HHV-7, as well as other viruses such as Epstein–Barr virus and cytomegalovirus,90.98. and 99. may increase the risk of an individual developing this reaction (see p. 619).100.101.102.103. and 104. The HHV-6 genome may become integrated into the host’s chromosomes. 105 Hypogammaglobulinemia may be associated with the reactivation of HHV-6.106.107.108. and 109. A blood eosinophilia is often present and this appears to result from increased levels of interleukin-5. 110 The occasional absence of eosinophilia calls into question the accuracy of the title DRESS syndrome. 111
The skin lesions include a maculopapular eruption, toxic epidermal necrolysis, Stevens–Johnson syndrome, and facial edema. It has been reported in a premature infant on phenytoin, 112 as well as in older children. 113 Type 1 diabetes mellitus, and the syndrome of inappropriate secretion of antidiuretic hormone may rarely develop as a consequence of the syndrome.114. and 115.
OTHER CLINICOPATHOLOGICAL REACTIONS
The following account details in alphabetical order the various clinicopathological patterns that have been associated with drugs. 19 The reader should refer to the appropriate page, listed for each reaction below, for an account of the clinical and histopathological features of each particular pattern and of the drugs that may be responsible.
Acanthosis nigricans
Various hormones and corticosteroids have been implicated in the etiology of some cases of acanthosis nigricans (see p. 504). There are no features that are specific for drug-induced lesions.
Acne
A number of drugs, cosmetics, and industrial chemicals may precipitate and influence the course of acne vulgaris (see p. 400). Sometimes, pustular acneiform lesions develop without the presence of comedones.
Alopecia
Numerous drugs have been implicated in the etiology of alopecia. Several different mechanisms may be involved (see p. 427). The best understood of these is the alopecia produced by the various antimitotic agents that interfere with the replication of matrix cells during anagen.
Bullous reactions
Blisters are an integral part of erythema multiforme, toxic epidermal necrolysis, and often fixed drug eruptions. Reactions resembling mucous membrane pemphigoid (see p. 164), pemphigus116. and 117. (see p. 135), and porphyria cutanea tarda (see p. 498) also occur. Bullae may develop in the course of drug-induced vasculitis or drug-induced coma (see p. 167). In addition to these circumstances, subepidermal bullae may also occur following the use of certain drugs (see p. 159).
Elastosis perforans serpiginosa
Lesions resembling elastosis perforans serpiginosa may be produced in patients receiving long-term penicillamine therapy (see p. 335).
Erythema multiforme
Drug-induced erythema multiforme is sometimes severe, with mucous membrane lesions and the clinical picture of the Stevens–Johnson syndrome (see p. 51). Target lesions are said to be less conspicuous in drug-related cases. The long-acting sulfonamides and various non-steroidal anti-inflammatory drugs are often implicated. 19
Erythema nodosum
Drugs have sometimes been implicated in the etiology of erythema nodosum (see p. 460). There are no distinguishing features of drug-induced lesions.
Erythroderma (exfoliative dermatitis)
Drugs are a significant cause of erythroderma, which usually commences some weeks after initiation of the drug (see p. 507). The rash often starts on the face and spreads over the rest of the body.
Fixed drug eruptions
There may be one or several sharply demarcated lesions, beginning as dusky patches, which fade, leaving an area of pigmentation (see p. 50). The lesion recurs in the same area after rechallenge with the drug. Urticarial and bullous forms have been described.
Granulomas
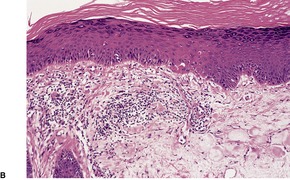
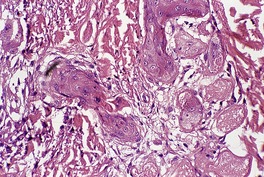
Rarely, a granulomatous tissue reaction is related to the ingestion of drugs, including the sulfonamides and allopurinol. Elastophagocytosis occasionally accompanies a drug reaction in sun-damaged skin. Granulomas may follow the local injection of various drugs, including toxoids containing aluminum salts. The interstitial granulomatous drug reaction is a distinctive clinicopathological entity (see p. 192) which histologically resembles the incomplete form of granuloma annulare (Fig. 20.3). 118
Fig. 20.3
Interstitial granulomatous drug reaction. There is a close resemblance to the incomplete form of granuloma annulare. (H & E)
Hypertrichosis
Hypertrichosis, usually facial, may occur with certain drugs, of which minoxidil and oral contraceptives are the most familiar. Occasionally the hypertrichosis is permanent, although it usually subsides following cessation of the drug (see p. 432).
Infarction
Hemorrhagic infarction of the skin is an uncommon complication of anticoagulant therapy (see p. 198). It usually occurs in the first week of therapy. 23
Lichenoid drug eruption
The lichenoid reaction resembles lichen planus to a variable degree (see p. 48). Sometimes there is a slightly scaly (‘eczematous’) appearance to the lesions. Postinflammatory pigmentation is more prominent than in lichen planus.
Lipodystrophy
A lipodystrophy has been reported in patients infected with the human immunodeficiency virus (HIV), following treatment with protease inhibitors (see p. 471).
Lupus erythematosus-like reaction
A disease resembling lupus erythematosus can be precipitated by several drugs (see p. 62). Procainamide-induced lupus erythematosus, which is the best studied, has a low incidence of renal involvement.
Neutrophilic eccrine hidradenitis
Neutrophilic eccrine hidradenitis is a rare complication of induction chemotherapy used in the treatment of certain types of cancer (see p. 439). Cytarabine has been the most frequently implicated drug.
Panniculitis
A panniculitis may result from the injection of certain drugs (see p. 476) and from the withdrawal of corticosteroids (see p. 469). Drugs including thiazides, sulfonamides, corticosteroids, oral contraceptives, and sulindac may cause a pancreatitis which in turn may be associated with a panniculitis (see p. 467). Erythema nodosum (see above) is a specific pattern of panniculitis sometimes associated with drug ingestion.
Photosensitivity
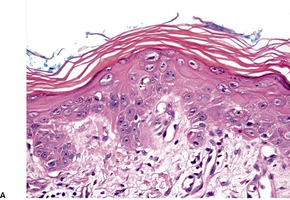
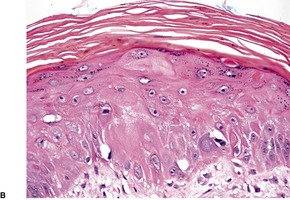
Although the lesions in the various stages of photosensitivity are most marked in areas exposed to the sun (Fig. 20.4), they sometimes extend to areas protected from the sun.119. and 120. Phototoxic and photoallergic variants have been recognized (see p. 535). Some persistent light reactions are drug induced (see p. 539).
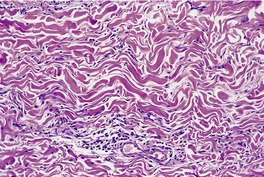
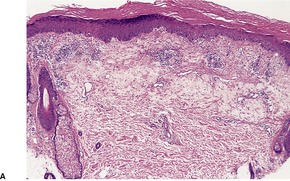
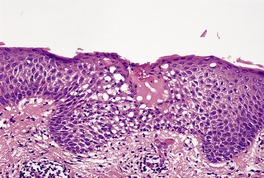
Fig. 20.4
(A) Photosensitive drug eruption. (B) There are rare apoptotic keratinocytes, solar elastosis, and stellate ‘fibroblasts’. (H & E)
Pigmentation
Several mechanisms are involved in the cutaneous pigmentation produced by drugs. These include an increased formation of melanin, melanin incontinence, and the deposition of drugs or drug complexes. 23 Antimalarials, phenothiazines, tetracycline and some of its derivatives, amiodarone, clofazimine, and various antineoplastic chemotherapeutic agents may all produce cutaneous pigmentation. Coadministration of minocycline and amitriptyline may accelerate cutaneous pigmentation. 121
Porphyria
Certain drugs may provoke attacks in those patients who have porphyria cutanea tarda or porphyria variegata, or in carriers of the genetic defect (see p. 497).
Drug-induced cutaneous pseudolymphoma is an uncommon reaction. It is seen most often with the antiepileptic drugs, 123 such as phenytoin and carbamazepine. It has also been reported with valproate sodium, atenolol, griseofulvin, imatinib, 124 ACE inhibitors, allopurinol, cyclosporine (ciclosporin), antihistamines, and mexiletine (see p. 1001). Pseudoclonality occurs in a number of cases so that interpretation of clonality studies needs to be correlated with morphology and clinical circumstances. 125 Resolution of the lesions takes longer than for other patterns of drug reactions with some cases persisting for 6 months or more, after cessation of the offending drug. 126
Psoriasiform drug reactions
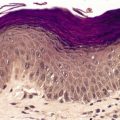
Various drugs, particularly lithium, may precipitate or exacerbate psoriasis (Fig. 20.5) and pustular psoriasis (see p. 81). The withdrawal of steroids may also precipitate pustular psoriasis. Sometimes the beta-blockers produce a clinical pattern resembling psoriasis although the histological picture is lichenoid or mixed lichenoid and psoriasiform in type. Acrodermatitis continua of Hallopeau has resulted from the use of terbinafine. 127
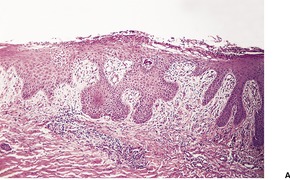
Fig. 20.5
(A) Psoriasis precipitated by the ingestion of lithium carbonate. (B) There is greater exocytosis of neutrophils and less regular psoriasiform hyperplasia than is usually seen in psoriasis. (H & E)
Purpura
Purpura may result from damage to the vascular endothelium, thrombocytopenia, or both. Vasculitis is another association although this produces a so-called ‘inflammatory purpura’; in the non-inflammatory purpuras there is simply an extravasation of red blood cells (see p. 196).
Pustular lesions
Pustules, usually resembling subcorneal pustular dermatosis on histopathological examination, have been reported with diltiazem, isoniazid, and cephalosporins (see p. 129). Subcorneal, intraepidermal, and even subepidermal pustules can be seen in acute generalized exanthematous pustulosis. Numerous drugs have been incriminated (see p. 132).
Sclerodermoid lesions
Sclerodermoid lesions may develop following occupational exposure to polyvinyl chloride and certain other chemicals, and following the use of bleomycin. Local sclerodermoid reactions may result from the injection of phytonadione (phytomenadione) or pentazocine (see p. 313).
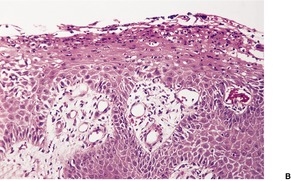
Spongiotic drug reaction following the ingestion of a thiazide diuretic. Note the conspicuous exocytosis of lymphocytes associated with the focus of spongiosis. (H & E)
Sweat gland necrosis
Sweat gland necrosis (Fig. 20.7) may occur in certain drug-induced comas (see p. 167).
Fig. 20.7
Sweat gland necrosis in a comatose patient from a drug overdose. Squamous metaplasia is developing in several glands. (H & E)
Toxic epidermal necrolysis
Toxic epidermal necrolysis is the most serious cutaneous reaction to drugs. Large areas of the skin are sloughed and this is usually preceded by the development of large flaccid bullae23 (see p. 53). Sulfonamides, allopurinol, and the non-steroidal anti-inflammatory drugs are most often implicated.
Ulceration
Ulceration is an extremely rare complication of drugs. Allopurinol has been incriminated in the formation of a foot ulcer, resulting from a peripheral neuropathy. 129 Hydroxyurea is another cause of leg ulceration (see p. 244).
Urticaria
Urticaria is second only to drug exanthems as a manifestation of drug reactions. Numerous drugs have been responsible (see p. 205). Insulin has become an uncommon cause of urticarial reactions, since the development of the contaminant-free, human preparations. 130 The mechanisms involved include IgE-dependent reactions, immune complexes, and the non-immunological activation of effector pathways involved in mast cell degranulation. 19
Vasculitis
The usual presentation of vasculitis is with ‘palpable purpura’ on the lower parts of the legs. 131 Immune mechanisms, particularly a type III reaction, are involved. Numerous drugs may produce a vasculitis (see p. 209).
Wound healing
Various drugs can influence wound healing. Adverse effects may be produced by corticosteroids, colchicine, cytotoxic drugs, and antibiotics. 132
OFFENDING DRUGS
The drugs which most often produce cutaneous reactions are the antibiotics, the non-steroidal anti-inflammatory drugs, psychotropic agents, the beta-blockers, and gold.1.4. and 133. Other important drugs are the thiazide diuretics, 134 antimalarial drugs,135. and 136. calcium channel blockers,78. and 137. ACE inhibitors, angiotensin II receptor antagonists, 138 phenytoin and derivatives, recombinant cytokines, 139 and anticancer chemotherapeutic agents. 140 Herbal remedies are an increasingly important cause of cutaneous reactions. 141
Some drugs have a low incidence of reactions. Knowledge of these drugs may assist in determining the offending drug in patients receiving multiple therapeutic agents. Drugs in this category include antacids, antihistamines, 142 atropine, digitalis glycosides, 134 insulin (regular), nystatin, potassium chloride, steroids, tetracycline, theophylline, thyroxine, vitamin preparations, and warfarin.23. and 31.
Brief mention will be made below of the major categories of offending drugs as well as the retinoids, recombinant cytokines, intravenous immunoglobulin, monoclonal antibodies, protease inhibitors, and botulinum toxin, all emerging areas of importance.
Antibiotics
Antibiotics are the major cause of drug reactions, accounting for 42% of all reactions in one series involving hospital inpatients. 4 Co-trimoxazole (trimethoprim-sulfamethoxazole) produced the highest number of reactions in one study (59 reactions/1000 recipients) while the frequency for ampicillin was 52/1000 and for the semisynthetic penicillins 36/1000. 5 In another study, amoxicillin resulted in the highest number of reactions (51/1000 patients exposed). 11 In a recent study of 472 children with rashes following antibiotic exposure, the frequency of an eruption was 12.3% for cefaclor, 2.6% for other cephalosporins, 7.4% for penicillins, and 8.5% for sulfonamides. 143 The macrolides (erythromycin, clarithromycin, roxithromycin, and azithromycin) have a low incidence of cutaneous side effects. 144
Other cutaneous reactions produced by antibiotics include an intertriginous eruption due to amoxicillin, 162 photosensitivity reactions with fluoroquinolones, 163 a severe anaphylactic reaction to topical rifamycin in a patient with hypersensitivity to ciprofloxacin, 164 and the ‘red man/red neck’ syndrome following the rapid infusion of vancomycin. 165
Adverse reactions have been reported to the new oral antifungal agents. Cutaneous reactions including urticaria, erythema, and pruritus have been reported in 2.3% of patients taking terbinafine.166. and 167. Isolated reports of erythema multiforme, toxic epidermal necrolysis, fixed drug eruptions, acute generalized exanthematous pustulosis, dermatomyositis, an erythema annulare centrifugum-like psoriatic drug eruption, a hypersensitivity reaction and alopecia, resulting from terbinafine, have appeared.168.169.170. and 171.
Many of these reactions have also been reported with the oral antifungal agents fluconazole and itraconazole. 166 In particular, itraconazole can produce acute generalized exanthematous pustulosis, a purpuric eruption, and erythematous papules,172.173. and 174. and fluconazole has been associated with erythema multiforme, toxic epidermal necrolysis, erythroderma, fixed drug eruption, and angioedema. 166 Beau’s lines have been reported on the digits following the use of itraconazole. 175 A hypersensitivity reaction has been produced by terbinafine. 93
The antiviral agent foscarnet produces penile ulcers in a high proportion of those who take it. Erosions of the vulva have also been reported. 176 A recall dermatitis restricted to the dermatomes previously affected by herpes zoster has followed the oral administration of acyclovir (aciclovir). 177 The ‘isotopic response’ is a similar phenomenon. 178
Non-steroidal anti-inflammatory drugs
The non-steroidal anti-inflammatory drugs (NSAIDs) are a chemically heterogeneous group of compounds that can produce a variety of cutaneous reactions ranging from mild exanthematous eruptions to life-threatening toxic epidermal necrolysis.179. and 180. They are among the most commonly prescribed class of drugs, accounting for approximately 5% of prescriptions dispensed in the United States.57. and 180. Several drugs in this category have already been withdrawn from the market because of their cutaneous reactions.
The following categories of non-steroidal anti-inflammatory drugs are in use: 180
• salicylic acid derivatives: aspirin and various compound analgesics
• heterocyclic acetic acids: indomethacin, sulindac, and tolmetin
• propionic acid derivatives: ibuprofen, naproxen, and fenoprofen
• anthranilic acids: mefenamic acid, flufenamic acid, and meclofenamate sodium
• pyrazole derivatives (pyrazolones): phenylbutazone and oxyphenbutazone
Drugs belonging to any given chemical group frequently share similar mechanisms of action and toxicity. The NSAIDs inhibit the enzyme cyclo-oxygenase and thus reduce production of prostaglandins and thromboxanes; this action is not solely responsible for their therapeutic actions. 57
Exanthematous eruptions are commonly seen with phenylbutazone and indomethacin but they have been reported at some time or other with most of the other NSAIDs. 19 Aspirin is an important cause of acute urticaria; it also aggravates chronic urticaria. 180 Ibuprofen may produce a vasculitis, morbilliform eruption, urticaria, erythema multiforme, erythema nodosum, a bullous eruption, or a lupus erythematosus-like eruption; 181 naproxen may produce a fixed drug eruption, a lichenoid reaction, or a vesiculobullous reaction. 180 Piroxicam may result in a vesiculobullous eruption in areas exposed to the sun. 57 It has also resulted in an aphthous stomatitis. 182 Most of the NSAIDs have been reported to cause toxic epidermal necrolysis and/or erythema multiforme at some time, although the substances most frequently responsible are the pyrazolones.19. and 57. The COX-2 inhibitors can produce a wide range of reactions ranging from exanthematous lesions through to urticaria and toxic epidermal necrolysis. Valdecoxib has been associated with a hypersensitivity syndrome reaction. 183 This class of drugs may give reactions with few, if any, eosinophils (personal observation).
Psychotropic drugs
The psychotropic drugs include the tricyclic antidepressants, antipsychotic drugs, lithium, and the hypnotic and anxiolytic (tranquilizer) agents. 184 This group of drugs produces the most diverse range of reactions, which include exacerbation of porphyria (chlordiazepoxide), blue-gray discoloration of the skin (chlorpromazine), and an acneiform eruption (lithium).184. and 185. Further mention of the specific complications of the various drugs in this category is made in the description of the appropriate tissue reaction.
Phenytoin sodium and anticonvulsants
Phenytoin sodium is a widely prescribed anticonvulsant with a relatively low rate of side effects. Nevertheless, a broad spectrum of cutaneous reactions has been reported. 186 These include exanthematous eruptions, acneiform lesions, exfoliative dermatitis, erythema multiforme, toxic epidermal necrolysis, vasculitis, hypertrichosis, gingival hyperplasia, coarse facies, heel-pad thickening, a lupus erythematosus-like reaction, digital deformities187 (the fetal hydantoin syndrome), a hypersensitivity syndrome,188. and 189. and a pseudolymphoma syndrome. 186 Carbamazepine, lamotrigine, phenobarbital (phenobarbitone), and primidone cause similar side effects to phenytoin sodium including a hypersensitivity syndrome – ‘the anticonvulsant hypersensitivity syndrome’.84.190.191.192.193.194. and 195. This syndrome is considered further with the drug hypersensitivity syndrome (see p. 515). Generalized pustulation is one manifestation of the syndrome.196. and 197. Phenytoin sodium has also resulted in cutaneous necrosis with multinucleate epidermal cells at the site of intravenous infusion. 198 Among the various medications in this group, carbamazepine is associated with the highest number of adverse cutaneous reactions (10–11%). 199
Gold
Gold produces a variety of cutaneous reactions which are most commonly ‘eczematous’ or maculopapular in type. 200 These reactions may occur as long as 2 years after the initiation of therapy. 19 The lesions may take months to resolve. 19 Other reactions produced by gold include cutaneous pigmentation, exfoliative dermatitis, vasomotor flushing, a lichenoid drug reaction, erythema nodosum, and an eruption resembling pityriasis rosea. 201
Retinoids are a group of compounds that produce their biological responses via a specific receptor whose usual bindings are retinol and retinoic acid. 207 Synthetic retinoids such as etretinate, tretinoin, and isotretinoin are of increasing importance in dermatological therapy. They have received widespread media coverage because of their ability to improve photoaged skin. They can also stimulate granulation tissue in chronic wounds, promoting wound healing. 208
Retinoids produce multiple changes, including a reduction in the keratin content of keratinocytes and in epidermal hyperplasia, and an increase in Langerhans cells, dermal collagen, tropoelastin, and angiogenesis. They produce reduced collagenase and gelatinase activity and glycosaminoglycans. 207
Retinoids appear to cause partial regression of established skin cancers and to inhibit the number of skin cancers that appear in susceptible individuals, such as those with xeroderma pigmentosum, as long as the treatment is continued. 207 The author was involved in an early clinical trial of retinoic acid, which was aborted when multilobate nuclei were found in the epidermis of individuals treated with topical retinoic acid for one year. This observation was never published.
Cutaneous side effects of synthetic retinoids include cheilitis, palmoplantar peeling, pyogenic granuloma-like lesions in acne, alopecia, and paronychia.207. and 209. Granulation tissue may form in the palpebral conjunctivae. 210 Induction therapy with all-trans-retinoic acid in patients with acute promyelocytic leukemia can produce a range of scrotal lesions including ulceration, exfoliative dermatitis, and Fournier’s gangrene.211. and 212.
Cytotoxic drugs
Cytotoxic drugs used in the treatment of cancer have many mucocutaneous complications. As combination chemotherapy is often used, it may be difficult to determine which drug is specifically responsible for a particular reaction. There is some evidence that some of the rashes attributed to drugs in the past may be examples of the eruption of lymphocyte recovery (see p. 57). It is still possible that a drug is responsible for these eruptions, in some cases, and that the reaction is only expressed when the number of immunocompetent cells returns to a sufficient level.213. and 214. Their action on rapidly dividing cells means that cytotoxic drugs commonly produce alopecia, stomatitis, apoptotic keratinocytes, and Beau’s lines on the nails.140. and 215. Chemical cellulitis, ulceration, and phlebitis may result from local extravasation into the tissues of injected drugs. 216 Vinca alkaloids, such as vincristine, vinblastine, and its semisynthetic analogue vinorelbine, have the highest potential for producing skin necrosis of all the anticancer drugs. 217
Other complications of cytotoxic drugs include alterations in cutaneous pigmentation (see p. 394), nail pigmentation, 218 neutrophilic eccrine hidradenitis (see p. 439), eccrine squamous syringometaplasia (see p. 438), sclerodermoid reactions (see p. 313), urticaria, vasculitis, erythroderma, inflammation of keratoses (see p. 678), 219 enlarged dermal macrophages, 220 and exacerbation of porphyria (see p. 497).140. and 215. Erysipeloid lesions are produced by the nucleoside analogue gemcitabine. 221 Pediatric patients sometimes develop an intertriginous eruption in association with various chemotherapeutic agents.222. and 223. Children receiving high-dose thiotepa, an alkylating agent, often develop a diffuse erythema followed by desquamation and hyperpigmentation. 224
An acral erythema (chemotherapy-induced acral erythema) has been reported from the use of certain chemotherapeutic agents, such as fluorouracil, doxorubicin, 225 cisplatin, 226 methotrexate,227. and 228. and cytarabine (cytosine arabinoside).229. and 230. The lesions subside within 1–2 weeks following discontinuation of chemotherapy, with eventual desquamation. The fixed erythrodysethesia produced by the combination of gemcitabine and epirubicin is probably a variant of acral erythema. 231 An erythrodysethesia with histological epidermal dysmaturation has also been produced by Doxil (see below). 232 A bullous reaction is rare.228.233. and 234. Acral erythema appears to be a common side effect of doxorubicin when it is encapsulated in liposomes (Doxil).219. and 235. Microscopic examination reveals mild basal vacuolar change, scattered apoptotic keratinocytes, and a mild superficial perivascular infiltrate of lymphocytes. 236 This formulation has also produced epidermal dysmaturation in intertriginous areas. 237 Eccrine squamous syringometaplasia is not uncommon. It has been suggested that natural killer cells initially target keratinocytes in the eccrine apparatus, producing small spongiotic vesicles adjacent to the acrosyringium, apoptosis of cells at all levels of the eccrine apparatus, and later squamous syringometaplasia. 238 Epidermal dysmaturation is sometimes produced (Fig. 20.8). 239
Fig. 20.8
Epidermal dysmaturation. (A) Some large epidermal cells are present. The patient had received chemotherapy a few weeks earlier. The biopsy was done for an associated drug reaction, subtle features of which are also present. (B) Dysmature keratinocytes are present at different levels of the epidermis. (H & E)
Intradermal bleomycin results in necrosis and apoptosis of epidermal keratinocytes and eccrine epithelium. There is an associated neutrophilic infiltrate around the sweat glands, resembling neutrophilic eccrine hidradenitis (see p. 439). 240 Bleomycin, peplomycin, and docetaxel may also produce a flagellate erythema followed by hyperpigmentation.241.242. and 243.
A linear, serpentine erythematous eruption overlying the superficial veins of both arms has been reported following the intravenous use of 5-fluorouracil.244. and 245. The changes have been called persistent supravenous erythematous eruption. A similar reaction limited to the arm of cytotoxic infusion has been produced by docetaxel. 246 The histological changes resemble erythema multiforme.
Subungual hemorrhages and abscesses have been reported as a side effect of docetaxel therapy.247. and 248. Extravasation of docetaxel during intravenous administration can produce a vesicant-like hemorrhagic eruption. 249 An exudative hyponychial dermatitis has also been reported with the combination of docetaxel and capecitabine. 250 A recall dermatitis has been induced by docetaxel at previous laser treatment sites. 251 Ultraviolet recall dermatitis developed in a patient receiving methotrexate and cytarabine. 252
Only gold members can continue reading. Log In or Register to continue