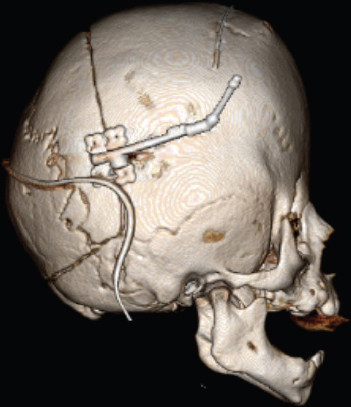
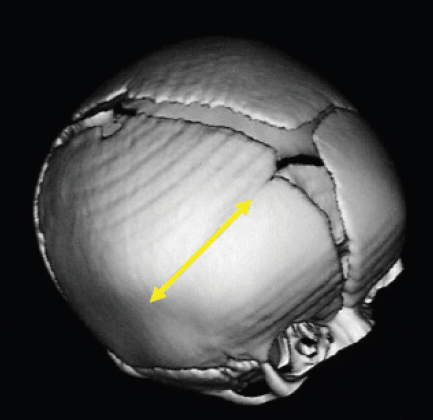
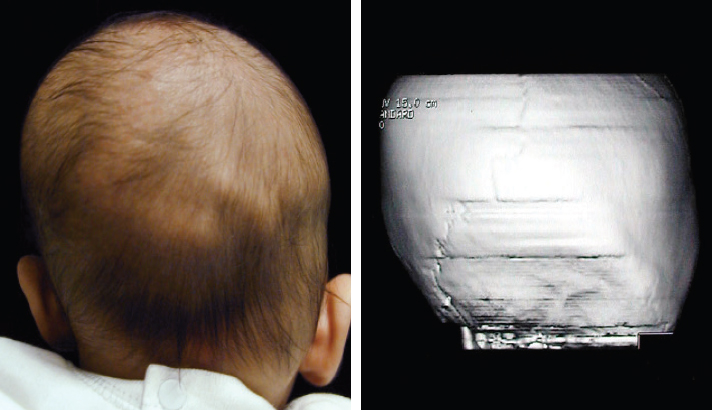
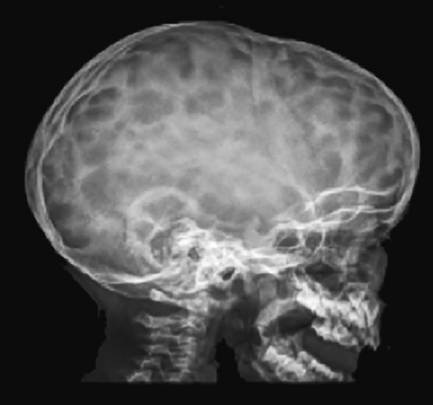
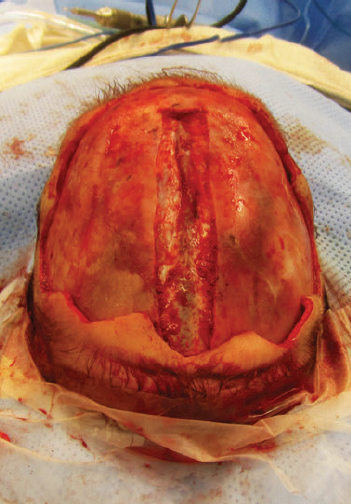
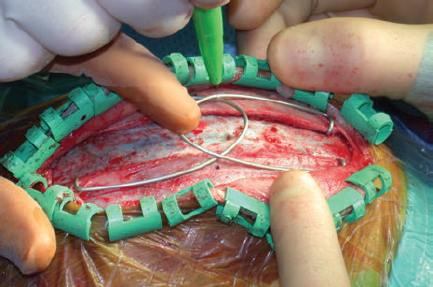
CHAPTER Normal skull growth and potential neurologic function may be affected by the presence of continued pressure in any one area of the cranium or by the presence of one or more pathologically fused cranial sutures. Posterior deformational plagiocephaly, most often secondary to a supine sleeping position, will generally resolve with positional changes, physiotherapy, or helmet therapy and is only rarely a surgical condition. The presence of a pathologically fused suture will produce deformity of the skull and is frequently an indication for operative release. The fused sutures determine the phenotype of the craniofacial deformity. According to Virchow’s Law, bone growth can no longer occur across (perpendicular to) the affected suture and therefore only occurs along it (parallel)1 (Fig. 41.1). Craniosynostosis can be classified into simple (single suture) versus complex (multiple sutures) and nonsyndromic versus syndromic subtypes. Assessment of an infant with an abnormal head shape includes a detailed medical history and physical examination to rule out a positional cause and identify any complicating sequelae. The medical history should identify any history of skull irregularities, associated syndromes, family history of calvarial deformities, and symptoms of intracranial hypertension (headache or vomiting, developmental changes, irritability, or oculomotor paresis). Often, parents note an abnormal head shape at the time of delivery or one that becomes more apparent later in infancy. Patients with irritability, feeding difficulties, failure to thrive, headache, developmental delays, visual changes, marked turricephaly, supraorbital recession, bulging or “tight” fontanels, abnormal distended scalp veins, or a lack of circumferential skull growth may have an increase in intracranial pressure. For patients with head shape abnormalities, a careful physical examination should be able to identify the cause. Positional deformation presents with a classic parallelogram appearance when looking from above. Skull deformation caused by premature fusion produces characteristic findings, including asymmetry (supraorbital retrusion, towering or turricephaly, frontal or occipital bossing), inability to palpate the anterior fontanelle (which normally remains open until 12 to 18 months of age), perisutural ridging, and signs of intracranial hypertension (papilledema). Studies have shown that the presence of intracranial hypertension is dependent on the number of affected sutures, ranging from approximately 14% for single-suture synostosis to approximately 47% in multisuture synostosis.2,3 Suture release in craniosynostosis is often offered to correct the craniofacial deformity and to address potential increased intracranial pressure that in some patients has resulted in blindness and developmental delay. Fig. 41.1 Virchow’s law: Bone growth can no longer occur across (perpendicular to) a fused suture and therefore only occurs along it (parallel). Fig. 41.2 Clinical lambdoid synostosis. The specific calvarial shape can indicate which sutures are involved. Children with sagittal synostosis present with a narrow, elongated skull (dolichocephaly describes long-headedness; scaphocephaly describes a boat-shaped head). Depending on the region of greatest fusion of the sagittal suture, the child may manifest frontal or occipital bossing or a combination of both. Some children will also demonstrate a “towering” skull, also known as turricephaly. Metopic synostosis is marked by a variable degree of phenotypic severity, ranging from mild ridging to the formation of a triangular head (trigonocephaly) or prominent “keel” forehead with or without hypotelorism. Although an endocranial ridge is not commonly seen in patients with metopic synostosis, an endocranial notch can be observed on axial CT images and is virtually diagnostic of pathologic suture fusion. Patients with unicoronal synostosis present with anterior plagiocephaly, whereas those with bilateral coronal involvement demonstrate brachycephaly. Phenotypic features of anterior plagiocephaly include ipsilateral perisutural ridging, forehead flattening, and orbital recession, coupled with contralateral compensatory frontal bossing. Facial deformities are also common, including nasal root displacement toward the ipsilateral side, anterior displacement of the ipsilateral ear, and chin deviation toward the contralateral side, resulting in a classic C-shaped craniofacial deformity—concave contralateral to the fused suture. Children with lambdoid synostosis characteristically have a trapezoid-shaped head (seen from the vertex view) in association with posterior displacement of the ipsilateral ear, contralateral occipital bossing, ipsilateral mastoid bossing, and ridging of the affected lambdoid suture. In contrast, posterior deformational plagiocephaly is marked by a parallelogram-shaped head when viewed from the vertex, anterior displacement of the ipsilateral ear, ipsilateral frontal bossing in the absence of palpable lambdoid suture ridge, and no mastoid bossing as is seen with lambdoid suture fusion (Fig. 41.2). Posterior plagiocephaly caused by lambdoid suture synostosis is rare; the majority of posterior plagiocephaly is secondary to positional molding. Understanding the phenotypic differences between lambdoid synostosis and posterior deformational plagiocephaly is critical for making the appropriate diagnosis and designing the proper course of treatment. Head circumferences, cranial indices, and anthropometric measurements should also be noted. Imaging studies may be necessary to confirm the diagnosis and rule out any associated intracranial abnormalities. For younger patients, ultrasonography has been used as a screening tool to visualize the sutures through the open fontanelles. Although not as sensitive as computed tomography (CT), it avoids the risk of radiation exposure. CT remains the most sensitive modality to assess bony sutural fusion and may suggest elevated intracranial pressure, as noted by areas of erosion of the inner calvarial table (“copper-beaten” appearance) (Fig. 41.3). Pathognomonic for unicoronal synostosis, elevation of the ipsilateral orbit can be seen secondary to superior displacement of the greater wing of the sphenoid, also known as the “harlequin” deformity. Modern CT protocols attempt to minimize the radiation dose to the infant.4 Both CT and magnetic resonance imaging (MRI) are helpful in evaluating the underlying brain for structural or functional abnormalities, including hydrocephalus, holoprosencephaly, cortical dysplasias, and Chiari malformations. The latter are structural defects in the part of the brain that controls balance (cerebellum). Without sufficient space, the cerebellum and parts of the brain stem may sit too low, causing pressure and blocking the flow of cerebrospinal fluid. This is important to identify preoperatively, because intraoperative maneuvers may worsen the condition. Fig. 41.3 Copper-beaten appearance of the inner table of the skull. Summary Box Common Complications in Synostosis Correction Intraoperative • Bleeding • Venous air embolism • Ocular injury and vision loss • Dural and brain injury, cerebrospinal fluid leak • Death Postoperative • Infection • Growing skull defects • Persistent calvarial defect • Hardware-related complication • Restenosis, relapse, growth restriction, and recurrence of deformity Surgical intervention is indicated in craniosynostosis to correct the craniofacial deformity and potentially treat or prevent functional disabilities believed to be secondary to intracranial hypertension (blindness, developmental de lay, psychosocial dysfunction). Patients with multisutural synostoses present with increased severity of physical and neurologic symptoms; therefore surgical intervention is even more important. The optimal surgical age has been debated, because the techniques of surgery are variable. Although the literature is inconclusive regarding the appropriate timing for correction of craniosynostosis, most craniofacial surgeons operate within the first year of age, taking into consideration the number and pattern of suture fusion, evidence of intracranial hypertension, and the surgical technique chosen. Minimally invasive techniques, which rely on less extensive craniotomies and external postoperative molding, are generally performed at an earlier age than are traditional open techniques. The technical portions of the procedures are complicated and have multiple risks. Avoidance of these risks is important to produce improved results. This begins with carefully evaluating potential patients preoperatively and optimizing their physical condition before surgery. In preparation for surgery, measures to ensure stable blood volumes should be undertaken. These include obtaining a baseline hemoglobin, blood type and crossmatch, and potential directed blood donation from a matched family member. Some surgeons use preoperative erythropoietin to minimize the need for transfusion.5 Surgery is performed under general anesthesia, which should be provided by a fellowship-trained pediatric anesthesiologist. Patients should be monitored postoperatively in an intensive care unit under the direction of pediatric critical care–trained physicians. A broad range of surgical options has been proposed for the surgical treatment of craniosynostosis. The goal of each is to remove the affected suture and either immediately remodel the remaining calvarial vault or provide postoperative guidance (distractors, springs, helmets) to allow this to occur. For most types of craniosynostosis repairs, patients are placed in the supine position to facilitate exposure. However, if the posterior vault is being addressed, as in a lambdoidal synostosis or some sagittal synostoses, the patient may be placed in the prone or sphinx position . In the prone position, care must be taken to ensure proper positioning with adequate protection of the eyes. Injury to the globe is devastating and should be a “never event.” Before the procedure begins, lubrication should be placed over the corneas; some surgeons approximate the eyelids with either adhesive tapes or formal tarsorrhaphy sutures that can be removed at the conclusion of the procedure. If the patient must be in the prone position, the face can be supported with a foam pillow or horseshoe headrest, with the eyes uncompressed within the opening of the support. Venous air embolism (VAE) is the introduction of air or gas from the operative field into either the arterial or venous vasculature and is a potentially fatal complication of neurosurgical procedures.6 Previous studies have suggested that the rate of VAE may be as high as 80% during such procedures. This may be lower for endoscopic techniques.7 Some believe that real-time monitoring, to identify the presence of a venous air embolism and allow for immediate intervention, mitigates the risk. Despite the introduction of newer diagnostic techniques, use of a precordial Doppler remains a standard modality. Although transesophageal echocardiography is the most sensitive method of detection,8,9 it is more costly and invasive. When properly placed between the third and sixth intercostal spaces along the right parasternal border, a precordial Doppler is potentially capable of identifying VAE at an air infusion rate as low as 0.015 mL/kg/min and consistently at a rate of 0.021 mL/kg/min.10,11 VAE may be graded by severity: change in Doppler tones (grade I), change in Doppler tones and decrease in end-tidal carbon dioxide (grade II), or decrease in systolic blood pressure by 20% from baseline (grade III). The calvarium is often approached via a standard “stealth” (zigzag) coronal incision, providing for adequate exposure while minimizing any postoperative scar. Perioperative antibiotics and steroids may be administered before the procedure. The incision is infiltrated with 1:200,000 epinephrine in 0.5% lidocaine to minimize bleeding along the incision site. The frontal and temporal regions are dissected in the subgaleal plane, and care is taken to preserve the periosteum on the surface of the bone, which helps minimize blood loss and may be used to stabilize the bony segments. Bleeding can occur at several points in the procedure. Incisions into the scalp can produce significant bleeding in the infant. This bleeding can be controlled with metal clips and cautery. Bleeding can also occur with elevation of the coronal flap. This is usually greater with subperiosteal dissection rather than supraperiosteal dissection. With either, punctate bleeding should be controlled with pinpoint cautery or bone wax. The latter should be used judiciously, because any wax left behind can serve as a nidus for infection. To “turn down” or reflect the coronal flap, the supraorbital vessels must be released from their attachments to the frontal bone. Sometimes, the vessels exit the bone through a notch; in older children they exit through a foramen. If the surgeon is not careful of these vessels, unnecessary bleeding can occur. When the vessels may exit through a foramen, a 2-mm osteotome should be used to convert the foramen to a notch by removing the inferior portion with the bony foramen. The vessels within the underlying periorbita can then be carefully dissected away from the bone. Performing the craniectomy involves making several small access holes and joining them with a side-cutting craniotome with a protective footplate. The access holes are made with a high-speed burr. Injury may occur if the burr is used too aggressively to enter the calvarial vault. The burr is often used to traverse the outer table, diploic space, and a portion of the inner table. As the remaining bone becomes thin enough, the burr can be put aside and communication to the epidural space made with a fine curette. Once a small opening is made with the curette, a Kerrison rongeur can be used to widen the opening further. The Kerrison has a protective footplate to minimize dural injury. Once the opening is large enough, a small elevator, such as a No. 4 Penfield, can be used to dissect beneath the bone and above the dura along the proposed craniotomy path. Once the bone cuts have been made, the bone flap should be removed carefully to avoid additional trauma to the underlying dura from sharp edges. The most severe bleeding can occur if there is injury to the sagittal sinus. The sagittal sinus is most at risk when the craniotome passes across the midline. For this reason, any cuts traversing the sagittal sinus are performed last. In the event of significant bleeding, the bone flap can then be removed relatively quickly to address the blood loss. With the remaining bone cuts already performed, the bone flap can be removed relatively quickly and any bleeding controlled. Injury to the sagittal sinus more posterior in the skull is more worrisome. The earliest approaches to treating craniosynostosis included simple suturectomy, allowing the brain to direct skull growth through the remaining open sutures. Inadequate correction prompted more extensive procedures of calvarial remodeling, and these have yielded improved results. These current techniques include wide scalp dissection, more remote calvarial osteotomies, and skull remodeling that is individually tailored to each cranial vault deformity.12 For sagittal synostosis, the surgical approaches range from minimal removal of the involved suture (usually combined with postoperative use of springs, distractors, or helmets) to extensive total calvarectomy and reconfiguration. Simple synostectomy, or simple strip craniectomy, when combined with postoperative springs, distractors, or helmet therapy, can be safe and well tolerated, providing adequate cosmetic results in select patients with mild deformities. Disadvantages include its lack of specifically addressing the severe compensatory changes in skull shape that result from the fused suture. It also leaves a large unprotected area over the vertex of the skull, an area with a high rate of restenosis and renewed growth restriction. The midvault “expanded strip craniectomy” provides a more immediate reconstruction of skull contour by shortening the anteroposterior dimension, expanding the biparietal dimension, and partially addressing the frontal and occipital prominences. The “Pi reconstruction,” a version of a midvault expanded strip craniectomy, is used for older infants (6 to 12 months of age) with scaphocephaly caused by sagittal synostosis (Fig. 41.4). Bone is removed lateral to the sagittal suture over the lateral parietal areas and molded, leaving two bony defects in the design of the Greek letter Pi (π). Cranial bone overlying the sagittal sinus is left intact to minimize bleeding. Axial compression is used to shorten and widen the skull, and absorbable plates are placed to hold the position. For coronal and metopic synostosis, the goal is to correct the frontal and orbital asymmetries. In the former, there is asymmetry in the shape of the orbits and forehead. In the latter, the typical deformity involves a midline ridge with retrusion of the supraorbital bar (“bandeau”) on either side of the forehead. The most common technique is fronto-orbital advancement (FOA). With an FOA, dissection continues within the orbits, freeing the periorbita off the upper half of the orbit. Caution must be taken to avoid injury to the underlying globes. To expose the roof of the orbits or anterior cranial base, a bifrontal craniotomy is marked and cut with an osteotome. Typically 1 to 2 centimeters of the superior orbital rim is left for support. The bone flap is placed aside and replaced in a more corrected position at the end of the procedure Fig. 41.4 Extended strip craniectomy for sagittal synostosis. Fig. 41.5 Spring-assisted cranioplasty. (This image provided courtesy of Lisa David, MD.) The supraorbital bar or bandeau is removed with careful osteotomies through the lateral orbit at the frontozygomatic suture, the superior orbit along the roof, and the nasion just above the nasofrontal suture. Care is taken to protect the underlying dura and brain as well as the orbital contents with adequate exposure and judicious use of retractors. This is a relatively low-risk maneuver but should similarly be performed with caution. The eyes are perhaps most at risk when cutting the orbital bandeau. Here, sufficiently wide malleable retractors should be placed between the globes and the saw blade or osteotome. The saw should not be run unless there is good protection of the underlying structures and the blade only advanced through the bone as far as needed. As the blade moves either medially or laterally, the retractors should follow to avoid inadvertent injury. The sphenoid wing is cut and the coronal sutures are opened to the level of the skull base to prevent continued growth restriction and resultant postoperative hollowing of the pterional regions. The bandeau is then reconfigured and fixed with resorbable sutures or plates and screws to maintain the newly contoured shape. Reconfiguration of the supraorbital bar might require osteotomies, both in the midline to flatten the forehead and laterally to normalize the lateral supraorbital angle. The goal is expansion on the affected side as well as recession on the contralateral side. When replaced, its lateral aspects and midline are fixed to the calvarial vault. This is performed for both unilateral and bilateral cases. To avoid relapse or a persistent deformity, overcorrecting the expansion of the affected side by 5 to 10% while also providing a convex shape at the lateral border is commonly necessary for a satisfactory reconstruction. The frontal bone flap is then attached to the supraorbital bar, taking care to match it to the previously overcorrected (5 to 10%) orbital bandeau on the affected side. For lambdoid synostosis, a variety of surgical approaches, aiming to release the affected suture(s) and normalize the posterior calvarial vault contour, have been described. Options include simple synostectomy, unilateral remodeling of the affected occipital region, and bilateral occipital reconstruction with or without the use of an occipital bandeau. Most lambdoid surgical candidates have significant parietal and frontal compensatory changes in addition to their occipital deformation; therefore they are best served by a more extended calvarectomy and remodeling. The reconstruction is similarly maintained with intervening bone grafts and resorbable hardware. Titanium was used early on but fell out of favor when it was noted that the plates translocated endocranially to the internal surface of the skull with calvarial growth. Resorbable plates made of polylactic acid provide temporary support across the osteotomy sites and dissolve within 12 to 24 months. After placement of the reconfigured supraorbital bar, the frontal bone is remodeled using the remaining portions of bone and fixed with absorbable plates or suture. Closure is performed in a routine fashion, with some surgeons placing subgaleal drains. To address concerns regarding incision length, operative blood loss, and length of stay associated with open cranio-facial procedures, minimally invasive techniques have been proposed. These techniques include endoscopic sutural release,13 spring-assisted cranioplasty14 (Fig. 41.5), and distraction osteogenesis15 (Fig. 41.6). Endoscopic release has been proposed to minimize the intraoperative risks by limiting the amount of bleeding from larger scalp incisions and bone flap elevation. The technique uses one or more small incisions, minimal dissection, and removal of the affected suture, possibly with adjunctive osteotomies into the surrounding bone. The technique does not attempt to completely correct the craniofacial deformity at the time of surgery but rather remove the offending sutures and allow remodeling during a period of postoperative brain growth, with or without external molding, or distractive force. The use of springs works in a similar fashion; the affected suture is removed and one or more internal springs are placed across the open osteotomy to guide remodeling of the skull (see Fig. 41.5). Of note, a second, smaller procedure is required to remove the springs. Similarly, distraction osteogenesis has been used to impart an internal force across the ostectomy site (see Fig. 41.6). New bone is laid down in the distracted osteotomy gap.
41
Craniosynostosis
Avoiding Unfavorable Results and Complications in Craniosynostosis
Preoperative Considerations
Surgical Considerations
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine