Cranioplasty is performed to restore the integrity and appearance of the skull. This most often involves the reconstruction of full-thickness skeletal defects. Cranioplasty may also be performed to normalize or to improve the contours of the intact cranium, usually the frontal area, and hence the appearance of the upper third of the face.
Acquired cranial bone deformities are usually full-thickness defects of the skull. In these situations, cranioplasty is done not only to normalize appearance, but also, and more importantly, to provide protection for the brain. Cranial defects may result from bone loss after trauma. The most common etiology of full-thickness cranial defects is infectious bone loss after elective access to the brain for neurosurgical treatment.
Historically, using either bone or alloplastic materials, the cranioplasty material was fabricated during the procedure. Over the last two decades, however, the use of computer-aided design/computer-aided manufacture (CAD/CAM) technology allows implants specifically for the needs of the patient to be prefabricated in anticipation of the cranioplasty procedure, thus improving the clinical result while saving operative time.
Skull Anthropometry
The position and shape of the forehead are largely responsible for the appearance of the upper face. The important aesthetic variables are its inclination, its relation to the globes, and the relative prominence of its frontal sinus. The brows and the frontal hairline are surface landmarks that overlie the frontal area. Their shape and location also have a powerful impact on facial appearance.
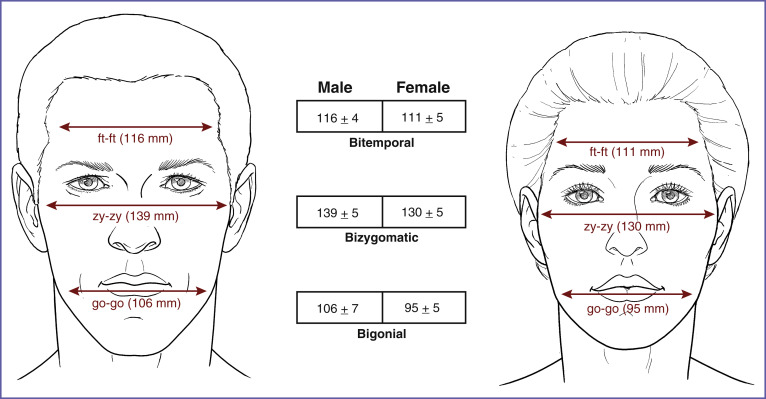
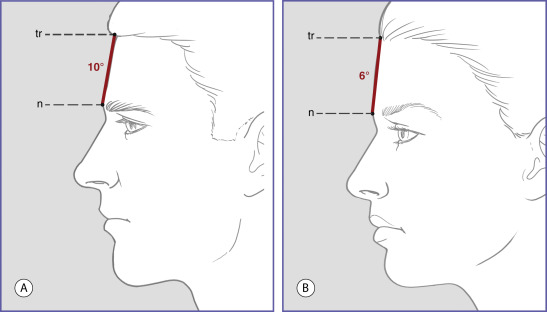
Normal values for certain dimensions of the frontal area are presented in Figs. 5.1, 5.2, and 5.3 . The bitemporal distance or width of the upper face is similar in men and women ( Fig. 5.1 ). Because men’s heads and their features are, on the average, larger than women’s, this implies that the upper third of women’s faces is relatively wide. The inclination of the forehead is more vertical in women than it is in men ( Fig. 5.2 ). More often in males, frontal sinus development creates a prominence in the central lower forehead that is absent or vestigial in females. In summary, when compared to men’s, the upper third of women’s faces is relatively flat, vertical, and wide. These values and relations should be kept in mind when reconstructing cranial defects or addressing aesthetic concerns in the frontal area.
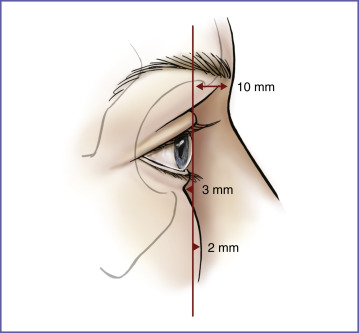
The relationship of the orbital rims to the globe is a primary determinant of the appearance of the upper one-third of the face ( Fig. 5.3 ). On the average, the surface of the soft tissues overlying the supraorbital rim lies 10 mm anterior to the cornea, while projecting 13 mm beyond the infraorbital rim. When the orbital rims have a greater projection beyond the anterior surface of the cornea, the eyes appear “deep set.” When the orbital rims project less, the eyes appear prominent. Certain craniosynostoses result in underdevelopment of the frontal bone and midface with marked projection of the globe beyond the orbital rims. When this disproportion is severe enough to cause symptoms due to corneal exposure or to be disfiguring, osteotomies are performed to allow skeletal advancement and improvement of globe–rim relationships. When globe–rim disproportions are less severe they are usually left untreated. Alloplastic augmentation of the orbital rims can be used to improve globe–rim relationships in patients with microform variants of congenital deformities or in “normal” patients with prominent eyes.
Cranioplasty for Full-Thickness Defects
Indications
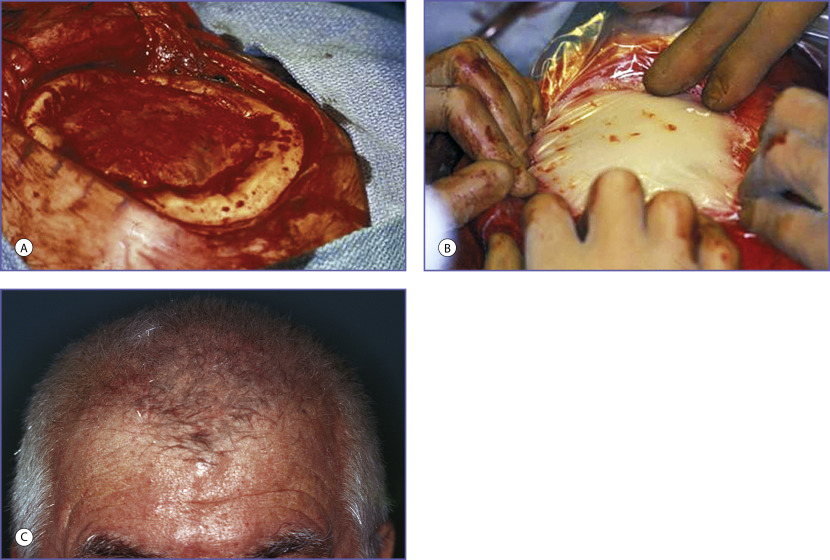
The most frequent indication for cranioplasty is the full-thickness skull defect resulting from the infectious loss of a craniotomy graft after elective craniotomy. A frequent cause of craniotomy graft (referred to as a “bone flap” by most neurosurgeons) loss results not from contamination at surgery but rather from wound-closure breakdown. This is precipitated by the common practice of making the osteotomy directly under the scalp incision. The resulting dead space directly beneath the suture line makes the soft tissue closure tenuous. The situation is further aggravated when plates and screws used to stabilize the replaced bone are positioned directly beneath the suture line. Minimal trauma can result in hardware and bone graft exposure with secondary infection ( Fig. 5.4 ). This can be avoided by planning the scalp flap well beyond the perimeter of the cranial osteotomy incisions. This avoids scalp incisions directly overlying bone incisions, as well as the possibility of fixation hardware being placed directly beneath the soft tissue closure.

In addition to its protective and contour-restorative functions, cranioplasty may also improve speech problems and hemiparesis if the skull defect is large enough to allow the scalp to exert direct pressure on the brain (“syndrome of the trephined”). Skull defects of greater than 2 or 3 cm should be considered for repair. However, this decision varies with location. Even small defects in the frontal area can be disturbing to the patient and therefore can be considered for repair.
Scalp incisions that directly overlie fixation hardware risk later wound dehiscence.
Cosmetic appearance alone can be an indication for repair such as small defects in the non-hair bearing and usually visible frontal area. On the other hand, small defects of the temporal and occipital areas, which are covered by thick muscle, are usually not reconstructed
Timing of surgery
Cranioplasty is performed when the soft tissue envelope is closed and acute infection as well as risk factors for recurrent infection are eliminated. This requires the removal of all devitalized tissues and any foreign bodies. Preparation requires the treatment of any frontal or ethmoidal sinus inflammatory disease. It also requires that any potential communications between the sinuses and the planned cranioplasty graft be eliminated. Large communications between the sinuses and the anterior cranial fossa, which may be the case after massive trauma requiring frontal sinus cranialization or after tumor removal, require placement of a vascularized barrier for effective isolation. A galea frontalis flap, if available and adequate, or a free tissue transfer may be required. Finally, the adequacy of the soft tissues to provide secure closure at the time of elective cranioplasty must be assured. This may require a preliminary scalp expansion or flap reconstruction before or at the time of cranioplasty.
A significant reduction in incidence of infection has been shown when 1 year is allowed to elapse between the initial injury or infection and the subsequent reconstruction. In the senior author’s experience, a 6-month infection-free period has been sufficient to assure that infection has been adequately treated.
Materials
Both autogenous bone and alloplastic materials are used to reconstruct the skull.
Bone is championed by many craniofacial surgeons because it becomes revascularized to varying extents by the host and therefore is less susceptible to infection and late complications. It has the disadvantages of requiring a donor site, being technically demanding and time-consuming to perform, exhibiting variable resorption, and therefore being prone to irregular contour. When bone is used for cranioplasty, resorption of between 25% to 40% has been demonstrated. Its use alone does not address the problem of intracranial dead space.
While craniofacial surgeons traditionally advocate the use of bone for cranioplasty, the vast majority of neurosurgeons use alloplasts, most often polymethylmethacrylate (PMMA). In reviewing the experience of 42 posttraumatic reconstructions of frontal defects in which both bone and acrylic were used, Manson et al. found that the material employed was not as important as the timing of reconstruction and the treatment of sinus disease. In the past, the senior author used bone when there had been recurrent infection or when overlying soft tissues were compromised (e.g., after radiation therapy). However, at present, he uses alloplastic materials almost exclusively for cranioplasty.
The alloplastic materials used for cranioplasty include PMMA, porous polyethylene, polyether ether ketone (PEEK), polymethylmethacrylate-polyhydroxyethylmethacrylate (HTR), titanium mesh, and hydroxyapatite.
The chemical composition and attributes of the alloplastic materials used for cranioplasty are detailed in Chapter 3 .
Implant fabrication at the time of surgery
At surgery, the patient is positioned so that a panoramic view of the skull and, if appropriate, the upper face can be draped into the field. This position allows the surgeon to mimic the contralateral anatomy and to avoid unnatural transitions. Preinjury photographs may be helpful. A skull model should be available to aid in the design of complex curvatures and landmarks.
Old scars are usually incised for exposure, and the scalp flap is removed carefully from the underlying dura. Any dural tears are repaired.
The exposed bone edge is saucerized by removal of the outer table with rongeurs or a high-speed burr. The resultant inner table ledge provides a ledge for implant placement and stabilization.
The most commonly used material fashioned at the time of surgery for skull reconstruction is PMMA. PMMA cranioplasty kits are available that contain a single dose of 30 g of powdered polymer and 17 mL of liquid monomer. The elements are mixed with a spatula in a bowl. The mixing should be conducted under ventilation so that the person mixing is not overcome by fumes. Mixing takes about 30 seconds. The bowl is then covered to avoid evaporation of the monomer. Doughing time varies with the temperature and is about 5 minutes at 72°F.
Two techniques are used to shape the implant. One method places the doughy mixture in a plastic sleeve provided in the cranioplasty kit. The sleeve containing the still-pliable implant mixture is placed onto the skull defect and molded by digital compression ( Fig. 5.5 ). The molding process occurs under continuous irrigation to avoid thermal damage to the dura and brain. A molding time of 6 to 8 minutes is usual. The exothermic polymerization process is allowed to take place away from the surgical field.