Summary and Key Features
- •
The stratum corneum is a dynamic structure that is continuously responding to a variety of daily exogenous factors that diminish its integrity and function.
- •
The term epidermal barrier is actually a collection of physiologic and homeostatic barrier functions, most of which correlate physiologically with normal stratum corneum structural and functional integrity.
- •
The stratum corneum (epidermal) permeability barrier is composed of two functioning components: (1) a cellular protein matrix and (2) an intercellular membrane matrix composed of a specifically arranged lipid bilayer. Proper function and maintenance of both components ensure skin integrity, epidermal water balance and hydration, and orderly corneocyte desquamation.
- •
Moisturizers are an important component of basic skin care and the management of many skin disorders, as they serve to counteract a variety of exogenous and endogenous factors that damage the stratum corneum permeability barrier and cause an increase in transepidermal water loss and a decrease in stratum corneum water content.
- •
Use of a well-formulated moisturizer or barrier repair formulation aids the inherent self-repair mechanisms of the stratum corneum and expedites permeability barrier repair by sustaining water content above the levels needed to maintain physiologic stratum corneum enzyme function; this ultimately preserves the structural and functional integrity of the stratum corneum permeability barrier.
- •
Well-designed barrier repair formulations, available by prescription but also found over the counter, are designed to include (1) fundamental ingredients that provide some magnitude of occlusivity, humectancy, and emolliency and (2) specific physiologic ingredients to augment innate barrier repair properties.
See and .
Introduction
The subject of epidermal barrier function in both healthy and diseased skin is very prominent in dermatology literature as new research aims to better understand the relationship between the barrier and disease. Clinicians are increasingly considerate of the importance of maintaining the structure and function of the epidermal barrier when treating patients and recommending over-the-counter (OTC) or prescription (Rx) products. In parallel, the skin barrier has become an increasingly familiar term to patients as proper skin care and the rationale for product selection are being discussed not only in the dermatology office but also on social media.
Previously, moisturizers were considered simple skin care with limited range, and relatively arbitrary rationale was applied for selection. However, there has been a marked increase in the complexity of moisturizer formulations, with many now recognizing the role of a moisturizer extends beyond transient hydration to also restore and maintain the structure and function of the skin barrier. While some moisturizers remain unsophisticated, it is the gold standard for well-formulated moisturizers to contain a combination of occlusive, emollient, and humectant agents. It is even commonplace for these products to incorporate specific ingredients designed to repair and maintain stratum corneum (SC) permeability barrier integrity and function and bring additional cosmetic benefits to the user. At the same time, there has been a considerable increase in more rigorous scientific evaluation of moisturizing products to demonstrate the efficacy of a given formulation beyond hydration. Evaluation methods employed include clinical assessments of skin condition in subjects with xerotic skin, SC hydration content (corneometry), analysis of SC ultrastructure (reflectance confocal microscopy, staining for structural proteins) and function (transepidermal water loss; TEWL), and incorporation of physiologic lipids in the SC (Raman spectroscopy or lipidomics via mass spectroscopy). With greater knowledge of how dysfunctions of the epidermal barrier contribute to the pathophysiology of specific skin conditions and with more scientific data emerging to support individual moisturizer formulations, clinicians are progressively able to give evidence-based and personalized recommendations to each patient. This chapter specifically covers moisturizers and barrier repair formulations, including the rationale for how they are designed and their application in clinical practice.
General Principles of Fundamental Skin Care
Why are well-formulated moisturizers and the maintenance of physiologic skin hydration integral components of the management of both healthy and diseased skin? To fully appreciate the answer to this question, it is important to recognize that while the epidermal barrier is a collection of physiologic and homeostatic barrier functions (discussed in detail in Chapter 1 ), central to overall epidermal barrier integrity and activity of the SC is the permeability barrier. The permeability barrier affects overall SC structural integrity and function and interacts with other SC barrier properties, and its impairment leads to insufficient and poorly balanced SC water content. An insufficient amount or improper distribution of water within the SC leads to diminished function of several enzyme systems that are needed to physiologically maintain basic epidermal/SC structure, physiologic desquamation, and normal skin elasticity and resiliency. This translates into skin surface roughness with visible scaling and flaking due to a buildup of corneocytes; increased skin rigidity, microfissuring, and macrofissuring caused by desiccation and shearing forces that are not counteracted due to diminished skin elasticity and resiliency; and localized areas of hyperkeratosis, especially on the hands, feet, and elbows.
While the SC is dynamic and continuously adapting and responding to its environment, a variety of exogenous and endogenous factors can diminish the integrity and function of the permeability barrier, resulting in an increase in TEWL and a decrease in SC water content. Thus fundamental skin care, namely cleansing, moisturizing, and photoprotection, which help protect and maintain the skin’s barrier, is integral to overall skin health and normal physiologic function of the SC. The focus of this chapter is on the role of moisturizers as an important component of basic skin care. When well formulated, moisturizers help restore skin’s water content and counteract and build resiliency against the exogenous and endogenous factors that damage the SC permeability barrier.
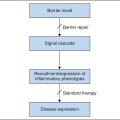
Exogenous factors that can impair the permeability barrier include the use of poorly formulated skin cleansers (e.g., those with alkaline pH or harsh surfactants), desiccating astringents (e.g., alcohol), topically applied irritants including certain topical medications (e.g., retinoids, benzoyl peroxide, corticosteroids), and low ambient humidity. Endogenous factors include mature age, chronic photodamage, and skin conditions inherently associated with clinical or subclinical alteration of the epidermal barrier and/or reduced SC water content, including forms of xerosis, atopic dermatitis, ichthyosis vulgaris, rosacea, and psoriasis. When SC permeability barrier impairment exceeds barrier repair through insufficient self-repair and/or inadequate moisturization, the SC becomes overstressed due to the prolonged increase in TEWL and decrease in skin hydration, leading to visibly xerotic skin, asteatotic dermatitis (i.e., eczema craquelé), and localized hyperkeratosis.
Now, to revisit the question originally posed: Why are well-formulated moisturizers and the maintenance of physiologic skin hydration integral components of the management of both healthy and diseased skin? A moisturizer not only restores moisture above the levels needed for physiologic SC enzyme function but also aids the barrier’s inherent self-repair mechanisms against exogenous insult and endogenous factors. Given this fundamental role and the myriad of moisturizer products available, it is critical to consider the composition of the formula and the scientific evidence in support of a product before recommending the product to patients as monotherapy or adjunctive care. The bottom line when evaluating a moisturizer formulation is to maintain a “simplest is best” approach and consider the physiologic needs of xerotic skin; to assist with this, it is beneficial to consider the SC’s natural mechanisms for maintaining skin integrity and water content.
Physiologic Maintenance of Skin Integrity and Water Content
Cutaneous water balance, homeostasis, and normal appearance of skin require an SC that is structurally and functionally intact. The epidermal permeability barrier consists of two functioning components: (1) a cellular protein matrix comprising an intertwined and layered lattice of corneocytes (“bricks”); and (2) an intercellular lipid bilayer matrix (“mortar”). Proper function and maintenance of both components ensures skin integrity, water balance, hydration, and orderly corneocyte desquamation. Disturbance of either or both of the SC functional components increases TEWL, resulting eventually in xerotic skin changes if not corrected. The ideal range of SC water content is 20–35%; reduction to <10% water content results in visibly evident xerotic skin changes, although even lesser changes in SC water content can trigger self-repair mechanisms, such as immediate release of preformed physiologic lipid precursors stored in the granular layer and an increase in filaggrin production, the predominant precursor of natural moisturizing factor (NMF).
Role of Corneocytes and Natural Moisturizing Factor
The SC is in constant flux, as corneocytes traverse from the lower layers of the SC and ultimately desquamate. The moisture content of corneocytes is maintained by small hygroscopic compounds that have been collectively categorized under the term natural moisturizing factor or NMF . The components of NMF, which include filaggrin-derived amino acids (i.e., arginine), pyrrolidone carboxylic acid (PCA), lactate, sugars, and several electrolytes, collectively serve as the innate humectants of the SC. NMF can be removed or reduced by cleansers, prolonged water exposure, the reduced production or processing of filaggrin, and other factors. If SC water content falls below a critical level, enzymatic function required for normal desquamation is impaired, leading to corneocyte adhesion and accumulation of corneocytes on the cutaneous surface. These aberrant changes correspond with the visible appearance of dryness, roughness, scaling, flaking, chafing, and fissuring.
Role of Intercellular Lipids
An important component of epidermal proliferation and differentiation is the formation of a permeability barrier composed of a programmed combination and ratio of lipids. SC lipids are synthesized predominantly within the nucleated cells of the epidermis and are largely autonomous from circulating lipids. Lipid synthesis is regulated primarily by changes in epidermal barrier status. Epidermal barrier lipids mostly comprise equimolar concentrations of free fatty acids, cholesterol, and ceramides. Lower quantities of cholesterol sulfate and nonpolar lipids are also present. The bipolar nature of lipids comprising the intercellular matrix (intercellular lipid membrane) allows for the formation of alternating lipid layers with hydrophilic “heads” and hydrophobic “tails.” This orderly arrangement forms a barrier that controls water permeability and movement between epidermal cells and corneocytes and seals water-soluble hygroscopic compounds (NMF) within corneocytes, thus maintaining the intracellular water content necessary for several SC enzymes to perform a variety of key physiologic and homeostatic functions.
Epidermal lipids are also collected within lamellar bodies, which are located within keratinocytes of the upper epidermis and function to biochemically convert newly synthesized lipids to an organized membrane structure (lamellar unit membrane structure). Lamellar bodies deliver proteolytic enzymes required for desquamation of corneocytes to the interstitium and convert precursor lipids into vital barrier function lipids (physiologic lipids) such as ceramides. As cornification occurs in the upper epidermis, a phospholipid-enriched plasma membrane is converted to a ceramide-rich bilayered membrane. Several subfractions of ceramides have been identified, accounting for up to 50% of SC lipid content by weight. Loss of epidermal lipids that are critical components of the lamellar epidermal barrier results in increased TEWL, a reduction in skin plasticity, and the adverse sequelae related to decreased SC water content as described earlier. Interestingly, significant reduction in multiple subfractions of ceramides has been noted in both lesional and nonlesional skin of patients with atopic dermatitis.
Physiologic Epidermal Barrier Repair
The homeostatic signal that correlates with maintenance and repair of epidermal barrier function is TEWL. When TEWL increases by as little as 1%, a physiologic signal initiates barrier repair by upregulating lipid synthesis. Disturbances in epidermal barrier permeability induce a physiologic response to restore barrier function, with normalization occurring within hours to days; the time course of restoration of barrier function is dependent on the extent of the insult, the age of the patient, and other factors.
Formulating an Effective Moisturizer
The “real-world” usage of a moisturizer formulation requires noticeable efficacy and cosmetic acceptability. With regard to efficacy, it is important to recognize that the term moisturizer does not imply that water is simply being added to the skin. Rather, a properly designed moisturizer formulation contains three fundamental types of ingredients—occlusives, humectants, and emollients—to address the xerotic skin changes induced by reduced SC water content. Today many OTC moisturizers and Rx barrier repair formulations go further to include additional additives that decrease TEWL and promote the maintenance of physiologic SC water content.
Types of Moisturizing Ingredients
Occlusives
Occlusive ingredients act by forming an artificial permeability barrier; they impede evaporation by forming a hydrophobic film. As they remain on the skin’s surface, occlusive agents provide perceivable benefit, but they can also often feel greasy to the touch. Examples of occlusive ingredients commonly found in moisturizers include petrolatum, lanolin, mineral oil, and silicone derivatives (e.g., dimethicone) ( Box 11.1 ). Each of these provides a variable level of occlusion to the skin. Petrolatum is the most effective occlusive but can be perceived as greasy even at reduced levels. Mineral oil is more fluid, which gives it a more favorable texture but limits its ability to reduce TEWL. Silicone derivatives are not greasy and impart a protective effect, making them the preferred choice for many formulations. Use of lanolin is limited by odor, expense, and potential allergenicity.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


