Summary and Key Features
- •
Atopic dermatitis (AD) and other eczematous skin conditions are accompanied by abnormal permeability barrier function.
- •
An equimolar mixture of three stratum corneum lipids is required for normal barrier function.
- •
These physiologic lipids account for the pool of lipids delivered to the stratum corneum.
- •
Nonphysiologic lipids do not penetrate the stratum corneum, and instead fully infiltrate the extracellular domains of the stratum corneum.
- •
Both physiologic and nonphysiologic lipids, alone and in combination, can be used as treatment for various skin barrier abnormalities.
- •
Emerging concepts regarding repair of barrier function, depending on the specific clinical indication, point toward the efficacy of (1) a combination of three physiologic lipids, or (2) a combination of one or more nonphysiologic lipids, such as petrolatum, or (3) vapor-permeable or vapor-impermeable dressings.
Introduction
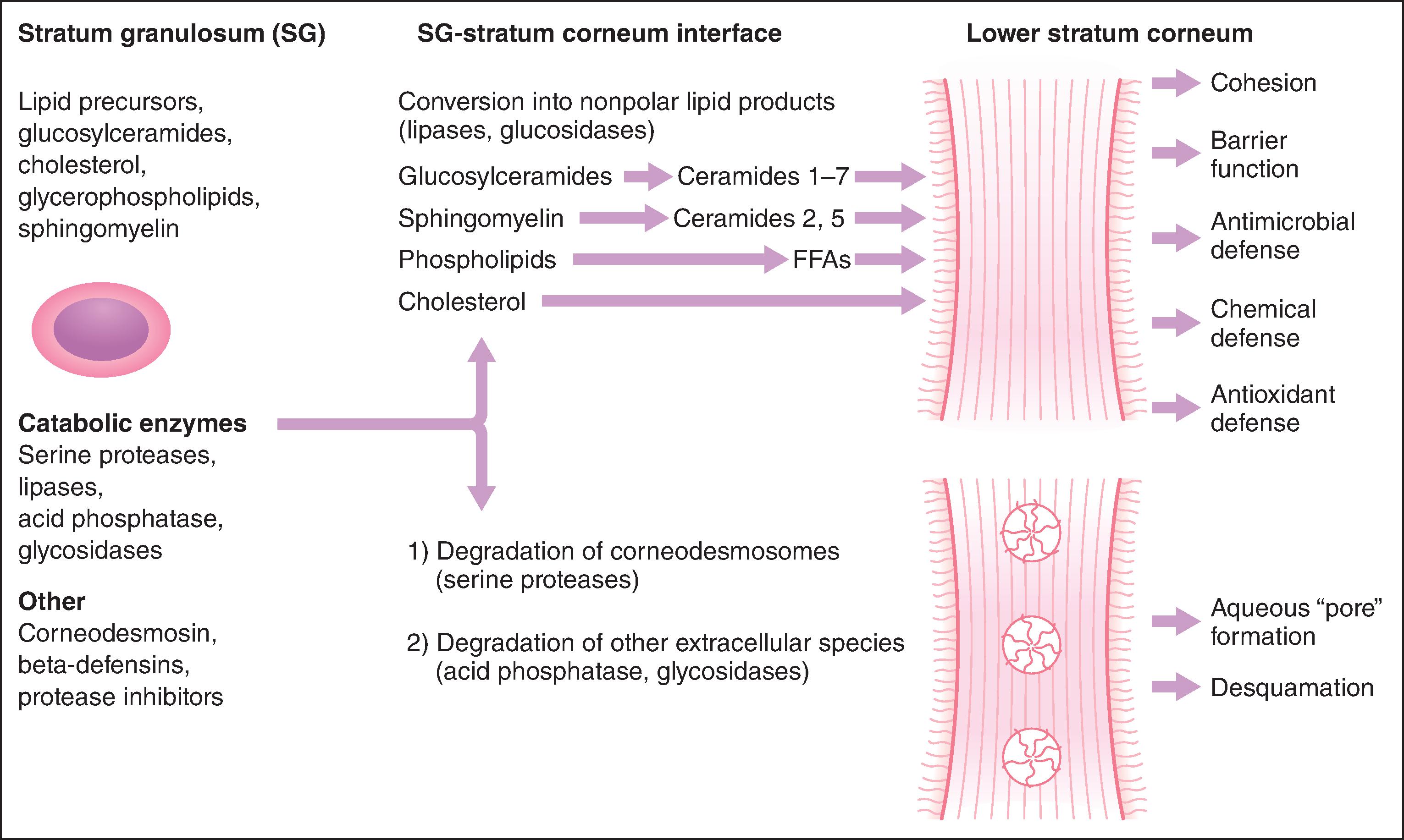
While the stratum corneum serves many defensive functions ( Table 7.1 ), none is as important as its ability to prevent excess loss of fluids and electrolytes from the body, that is, its permeability barrier. Permeability barrier function is mediated by the organization of three extracellular lipids of the stratum corneum into a series of parallel lamellar membranes, which mediate not only permeability barrier function but also additional, key protective functions of the epidermis ( Fig. 7.1 ). The defensive functions of the stratum corneum further localize to the cellular (corneocyte) compartment, or the extracellular matrix, or to certain features of both compartments ( Table 7.1 ).
| Function | Localization |
|---|---|
| Permeability barrier a | Extracellular (stratum corneum) |
| Initiation of inflammation (cytokine activation) a | Corneocyte cytosol (and granular cells) |
| Cohesion (integrity) → desquamation a | Extracellular (stratum corneum) |
| Antimicrobial barrier (innate immunity) a | Extracellular (stratum corneum) |
| Mechanical (impact and shear resistance) | Corneocyte envelope and corneodesmosomes |
| Toxic chemical/antigen exclusion | Extracellular (stratum corneum) |
| Hydration | Extracellular and corneocyte cytosol |
| UV barrier | Corneocyte cytosol ( trans -urocanic acid) |
| Neurosensory interface | Granular layer |
Dynamics of Barrier Recovery
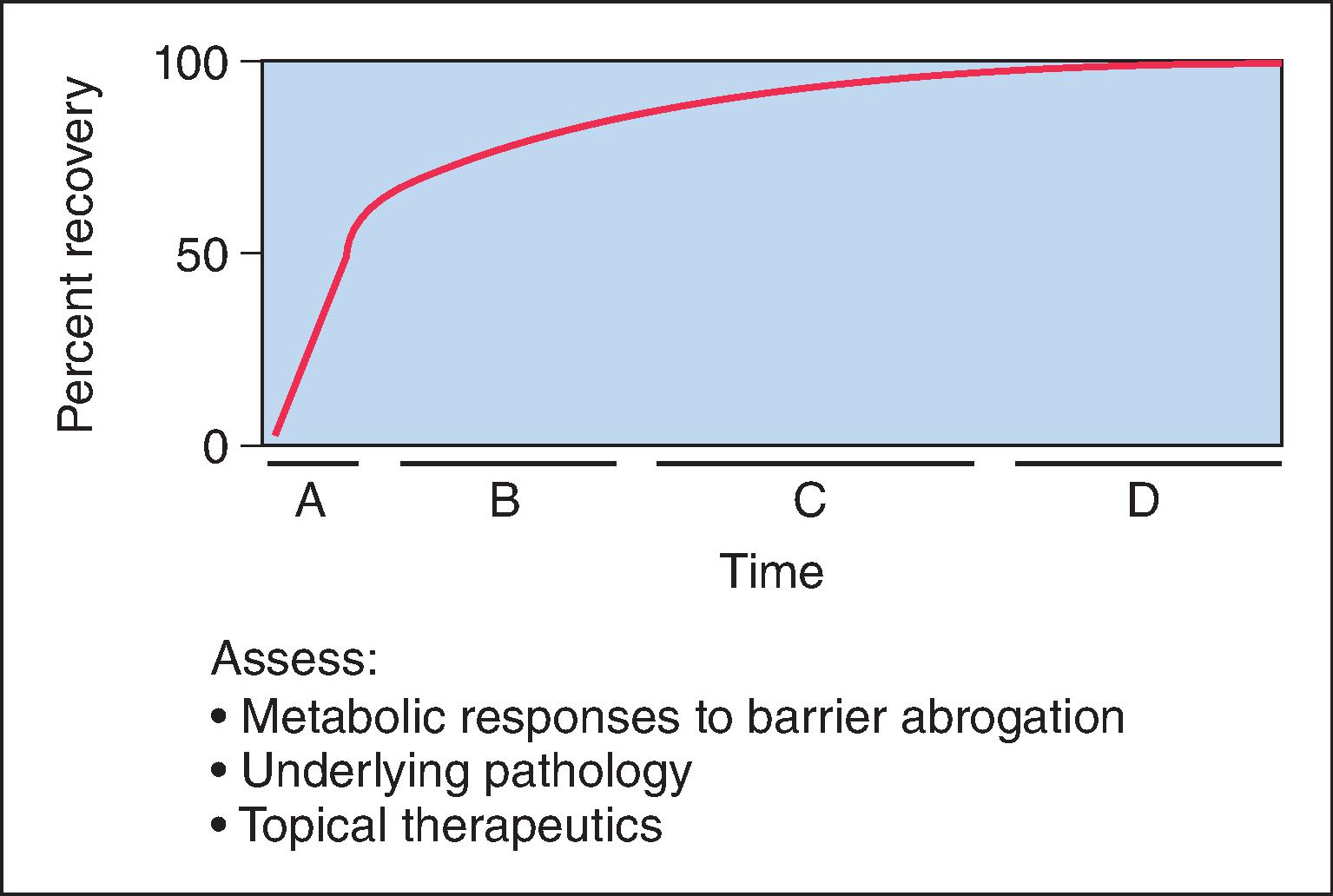
The skin barrier is assaulted frequently in daily life by hot water, detergents, solvents, mechanical trauma, atmospheric free radicals, and occupation-related chemicals. If these insults are widespread and repeated frequently, and/or if the host’s repair response is insufficient, they can threaten the organism with desiccation due to accelerated transepidermal water loss (TEWL). To avoid this outcome, the underlying epidermis mounts a coordinated metabolic response, ranging from increased lipid synthesis to accelerated lipid secretion, aimed at rapidly restoring normal function. This response is elicited by any type of barrier insult (e.g., organic solvents, detergents, tape stripping) that depletes the stratum corneum of its complement of lipids. Although the total time required for barrier recovery varies according to age, an initial, rapid recovery phase leads to 50–60% recovery in young healthy humans by about 12 hours, with full recovery requiring about 3 days ( Fig. 7.2 ). But in aged healthy humans (> 75 years), complete recovery from comparable insults is prolonged up to about 1 week. Restoration of barrier function is accompanied by reaccumulation of lipids, visible with either oil red O staining or Nile red fluorescence, and by the reappearance of lamellar membrane structures within the stratum corneum interstices, as early as 2 hours after acute disruption. Because artificial restoration of the barrier with vapor-impermeable membranes totally inhibits barrier recovery as well as all the metabolic processes linked to it, this entire series of responses is aimed specifically at restoring normal permeability barrier homeostasis. An impermeable membrane sends a message that the barrier is okay, even though the underlying barrier has not been restored.
Clinical Applications of the Cutaneous Stress Test
The kinetics of barrier recovery after acute perturbations (also called the cutaneous stress test) can discern abnormal function or underlying pathology even when basal parameters are normal ( Fig. 7.2 ), analogous to the cardiac treadmill exam. Indeed, the cutaneous stress test reveals deficient barrier function both in aged and neonatal skin, despite deceptively normal function in both age groups under basal conditions. Further, it amplifies differences between other ”normal” groups:
- •
Testosterone-replete versus testosterone-deficient humans
- •
Prolonged exposure of skin to humid versus dry environments
- •
Humans with dark versus light pigmentation
Finally, humans and animal models subjected to increased psychological stress reveal a glucocorticoid-mediated defect in barrier function. These findings could explain the propensity for the skin to erupt in inflammatory dermatoses, such as psoriasis and atopic dermatitis, in humans who are subject to psychological stress.
Lipid Composition of Lamellar Membranes
The extracellular lipids in the stratum corneum derive primarily from the secreted contents of epidermal lamellar bodies (LBs), which are enriched in cholesterol, glucosylceramide, and phospholipids, as well as their corresponding hydrolytic enzymes ( Fig. 7.1 ). These acidic, pH-dependent, lipid-processing enzymes catalyze the extracellular degradation of sphingomyelin and glucosylceramides to ceramides (Cer) and phospholipids to free fatty acids (FFAs), which, along with cholesterol (Chol), form the lamellar membranes required for permeability barrier homeostasis. Thus the stratum corneum lamellar membranes are composed of unique biologic membranes that mediate the barrier because of:
- •
Their extreme hydrophobicity (their free and esterified fatty acids are very long chain and highly saturated)
- •
The total weight percentage of lipids in the stratum corneum equaling the number of lamellar bilayers in the extracellular spaces (the more stacks, the better the barrier), which normally amounts to 10% of stratum corneum mass
- •
Their presence in an equimolar mixture of Cer : Chol : FFA
- •
The presence of certain Cer, that is, acylceramides, bearing linoleic acid, which tether the lamellar bilayers to each other
Together, these characteristics largely explain the barrier properties of the stratum corneum.
Lipid Synthesis and Requirements for the Barrier
The formation of epidermal LB requires a coordinated synthesis of the precursors of the three major lipids in the stratum corneum: cholesterol, glucosylceramides, and phospholipids. Although the epidermis is a very active site of lipid synthesis even under basal conditions, permeability barrier disruption stimulates a further, marked increase in the synthesis of Chol, Cer, and FFA, which provides the pool of lipids that is required for the formation of new LB. However, synthesis of these lipids is not only regulated by barrier requirements; it is also required for normal function. Using specific inhibitors of key lipid synthetic enzymes, we demonstrated an individual requirement for Chol, FFA, Cer, and glucosylceramide synthesis for barrier formation. In fact, blockade of these enzymes always produces a similar result: decreased LB contents and a paucity of extracellular lamellar bilayers. Thus each of the three families of stratum corneum lipids is required individually for permeability barrier function.
Equimolar Distribution of the Three Key stratum corneum Lipids
Whereas the previously described studies clearly demonstrate the individual requirement for Chol, Cer, and FFA for the permeability barrier, when each of these lipids is applied topically to damaged skin, the barrier gets worse! Instead, all three species must be supplied in an approximately equimolar mixture for normal barrier recovery to occur ( Table 7.2 ). For example, topical applications of any one or two of the three key lipids to acutely perturbed skin actually delays barrier recovery ( Table 7.2 ). Both incomplete and complete mixtures of the three key lipids rapidly traverse the stratum corneum and internalize within the granular cell layer, targeting the trans-Golgi network, where LB are formed ( Fig. 7.3 ). Exogenously applied and endogenous lipids mix within nascent LB, producing normal or abnormal LB contents and lamellar membrane structures, depending on the molar distribution of the applied lipids. Barrier recovery can be further accelerated by increasing the proportion of any one of the three key lipids to a 3 : 1 : 1 ratio ( Table 7.2 and Fig. 7.4 ). Thus physiologic (meaning characteristic of an organism’s healthy or normal biological functioning) mixtures of topical lipids influence barrier function, not by partially occluding the stratum corneum, as do nonphysiologic (meaning not naturally occurring) lipids (discussed shortly), but rather by contributing to the pool of epidermal lipids that is delivered to the stratum corneum interstices.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


