Introduction
Gynecomastia is defined as benign glandular enlargement of the male breast, its hallmark location being a concentric mass directly beneath the nipple. , It can consist of various proportions of excess subareolar fibrous breast and adipose tissue peripherally, and its extent depends on the individual’s body habitus. By contrast, pseudogynecomastia is enlargement of adipose tissue of the male breast. Gynecomastia is by far the most common breast problem in men, with an overall incidence of 32%–36% with up to 75% of cases being bilateral.
Physiologic temporary overgrowth of the adolescent breast also can be responsible for gynecomastia. With onset at approximately age 14 in more than 65% of healthy boys, gynecomastia typically resolves within 2 years. Persistent adolescent-onset gynecomastia beyond age 21 is unlikely to resolve with conservative management.
Gynecomastia also can manifest in men of advanced years. In middle-aged and older men, it is most commonly due to the excessive aromatization of androgens to estrogens, resulting in a decreased overall level of circulating testosterone. It may manifest in 40%–50% of men over 40 years of age.
Although most patients with gynecomastia present with cosmetic concerns, symptomatic gynecomastia can be characterized by breast pain and tenderness. In this chapter, the authors describe their preferred techniques for surgical treatment of gynecomastia to ensure an optimal outcome but with minimal scarring. In addition, patient selection and preoperative evaluation are also described.
Indications and Contraindications
Most patients present with cosmetic concerns about their breast appearance or chest contour. Some patients may complain about breast pain and tenderness. Therefore, surgery is usually indicated to correct gynecomastia related to a breast or chest contour problem.
Contraindications for surgical correction of gynecomastia include any medical conditions that cause such a condition. Therefore, a complete endocrine workup and certain imaging studies are required for all patients to identify endocrine disorders or tumors related to the testicles, adrenal gland, or pituitary gland. In addition, thyroid, renal, or liver function and medications taken by patients should be evaluated.
Preoperative Evaluations and Special Considerations
Initial evaluation requires a detailed history and physical examination to differentiate among fatty tissue, parenchymal enlargement, and a tumor. Age of onset, duration, symptoms, medications, recreational drug use, and medical history are key components to the initial evaluation. The breast examination assesses for fatty versus glandular predominance, excess breast skin, breast ptosis, and palpable masses. In addition, male breast cancer also should be ruled out.
Classification schemes exist to better define the extent of gynecomastia and dictate surgical treatment. The Simon classification has traditionally been employed (types I–III), as follows :
- I.
Small but visible breast development, without skin redundancy
- a.
Moderate breast development without skin redundancy
- b.
Moderate breast development, with skin redundancy
- a.
- II.
Severe breast development with large skin redundancy
The senior author acknowledges this classification with the following modification, which more directly correlates subtype with surgical strategy:
- •
Core breast tissue only: Direct excision
- •
Primarily fatty chest tissue: Ultrasound-assisted liposuction (UAL)
- •
Both core breast tissue and fatty chest tissue: First stage—UAL; second stage—direct excision in 6 months
- •
Fatty chest tissue and excess breast skin: First stage—UAL; second stage—periareolar mastopexy in 6 months
Nipple position, size, and sensation also must be assessed.
The normal average areolar diameter in the male nipple–areola complex is 25–30 mm, and these dimensions may be affected in cases of gynecomastia. The areola circle must also be addressed and may require a reduction in size or correction in the case of nipple herniation. Finally, mammography or even biopsy may be indicated in certain patients.
Complications are generally rare and well tolerated, but risks of overresection or underresection should be disclosed to patients preoperatively to manage expectations, facilitate informed consent, and provide anticipatory guidance for secondary revisions.
Surgical Techniques
Relevant Surgical Anatomy
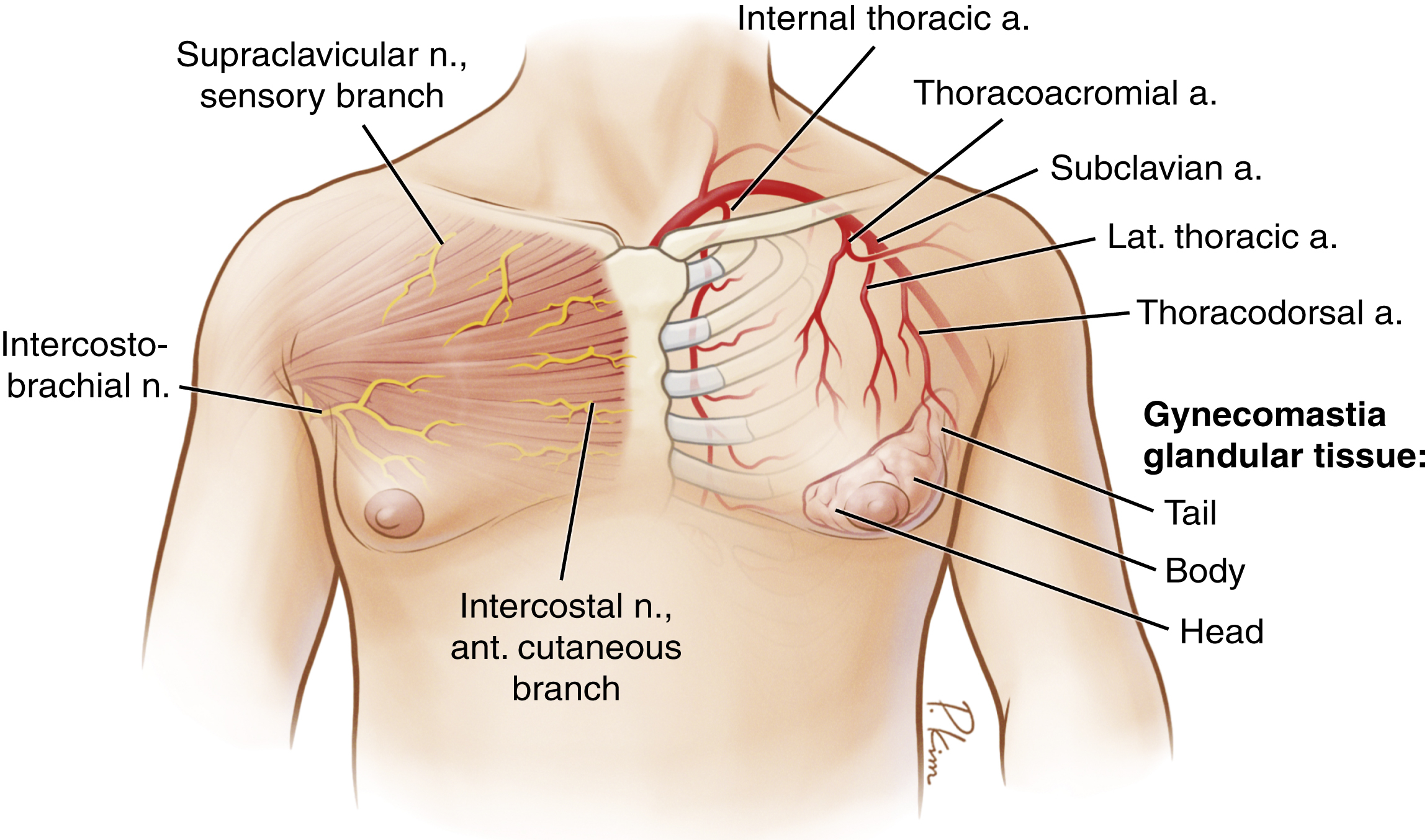
The blood supply of the male breast is the same as that in the female breast. The nipple is primarily innervated by the medial and lateral branches of the fourth intercostal nerve. However, the third and fifth intercostal nerves also may contribute. Gynecomastia in males is composed of the core, body, and even tail of glandular breast tissue ( Fig. 23.1 ). Each part of breast tissue can be quite different in terms of its characteristics. For example, the core breast tissue is usually directly under the nipple–areola complex and can be hard and difficult to remove even by UAL. In addition, patients may have excess breast skin and even natural breast ptosis similar to those in the female breast.
The goal of surgical correction for gynecomastia is to restore normal male chest contour but not eliminate all breast tissues. A wide variety of surgical treatment options for removing redundant male breast tissue have been described in the literature, including direct excision, traditional or ultrasound-assisted liposuction, combination of liposuction and direct excision, and use of an arthroscopic shaver.
Direct Excision
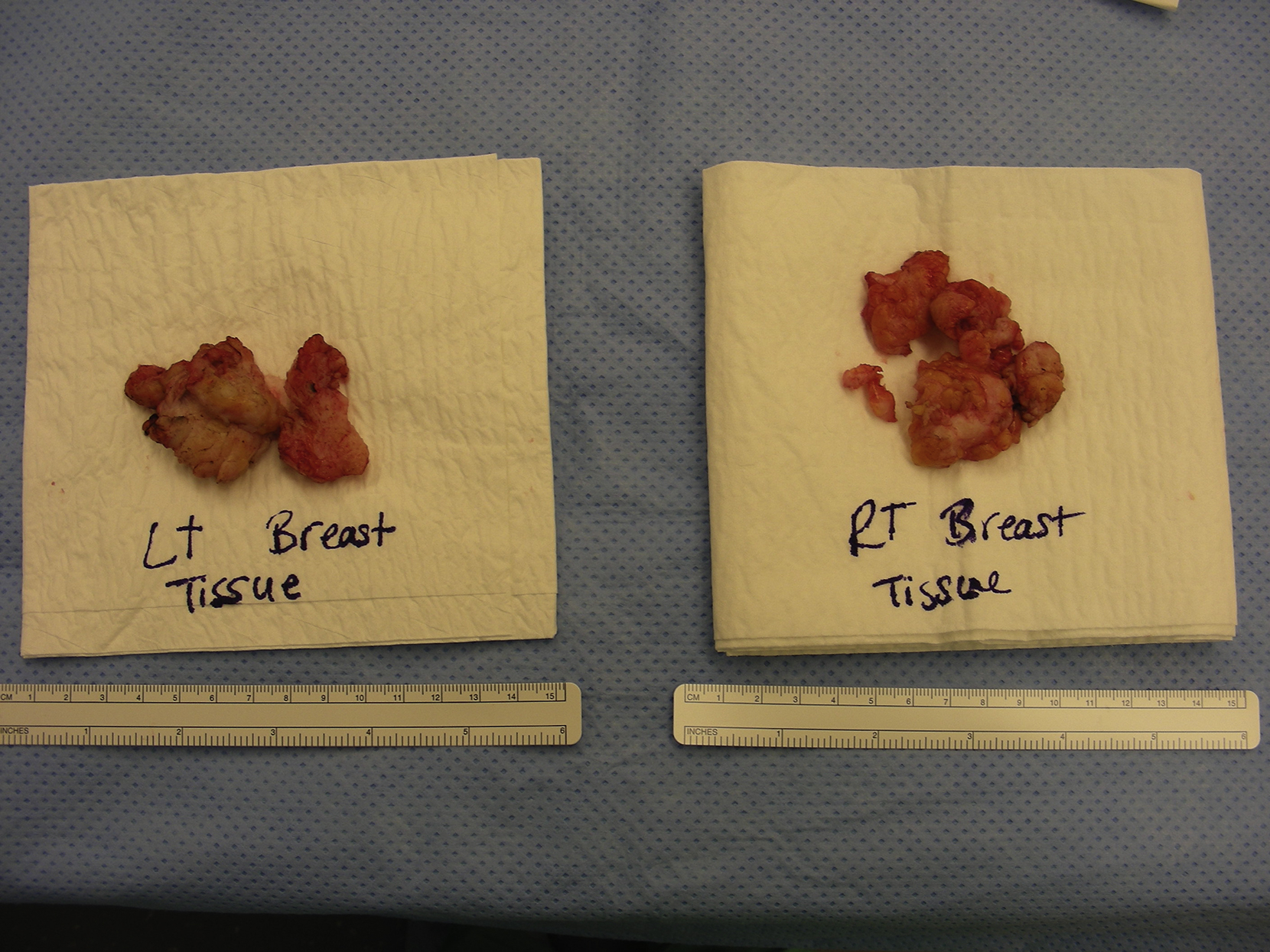
For patients with enlarged core breast tissue only, a direct excision of subareolar core breast tissue through a limited areolar incision combined with a pull-through technique can be a reasonable approach. Periareolar incision can offer a direct access for tissue resection ( Fig. 23.2 ). After the exposure of subareolar core breast tissue, it can be removed via a pull-through technique ( Fig. 23.3 ). Attention should be given to preserve adequate core breast tissue (approximately 0.5 cm in thickness) under the nipple so blood supply to the nipple is not compromised and noticeable nipple depression can be prevented.

Ultrasonic-Assisted Liposuction
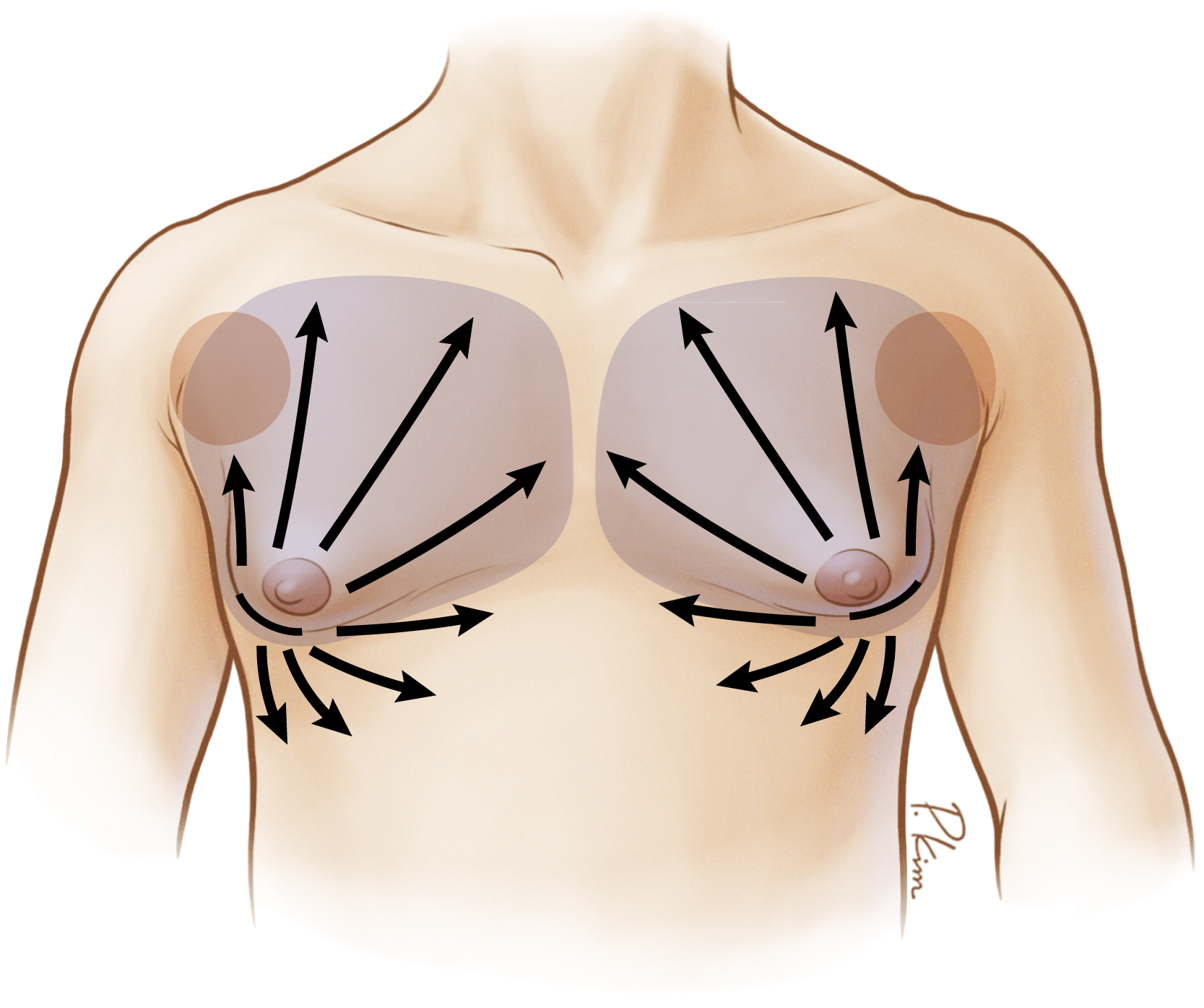
Most gynecomastia tissue is glandular; therefore, traditional liposuction is less effective used as a primary option for treating gynecomastia. Therefore, UAL is a valuable tool in the plastic surgeon’s armamentarium in treating gynecomastia. The basic tenets of UAL include infiltration of a super-wet solution, a stab incision at the inferolateral aspect of the chest, employing a radial pattern of suctioning across the entire chest ( Fig. 23.4 ), and disrupting fibroglandular tissue through cavitation of cells in tumesced fields. In addition, UAL may have an advantage in promoting skin retraction, so for cases with mild to moderate ptosis an external scar can be eliminated or minimized for correction of gynecomastia.
Once the patient is marked in an upper right position and excess breast tissue is outlined ( Fig. 23.5 ), a super-wet solution is infiltrated into the breast; the amount of infiltration is recommended by the manufacturer according to the proposed ultrasonic time (1.5 minutes per 100 cc solution) if UAL is performed ( Fig. 23.6 ). If the new-generation Vaser system (Sound Surgical Technologies, Louisville, CO, United States) is used, a five-ring probe with 90% continuous mode should be used ( Fig. 23.7 ). The probe should be moved slowly and consistently without pause, and adequate ultrasonic time is needed to maximize the destruction of fibroglandular breast tissue ( Fig. 23.8 ). After adequate ultrasonic cavitation on the tissue, conventional liposuction is performed vigorously to move all lipoaspirates ( Fig. 23.9 ). Once liposuction is completed, all remaining fluid should be milked out and the incision is closed ( Fig. 23.10 ). The chest is then covered with heavy tape for compression and contouring ( Fig. 23.11 ). A pressure garment should be used routinely for all patients after UAL.