The muscles that attach to the pubic bone (rectus abdominis, adductor longus, pectineus, and adductor brevis) constitute a harness that serves as the bedrock of core stability and underpinning the athleticism that defines performance in sports. Their attachment to the pubic bone is a point of weakness that, when disrupted, results in pain and a loss of athleticism. These injuries are not uncommon in baseball. A comprehensive understanding of their function and the commonality of injuries in this area is crucial for developing effective interventions aimed at enhancing athletic longevity and minimizing the risk of injury.
Key points
- •
A core muscle injury refers to any injury involving the muscles from the chest to the mid-thigh and they are not uncommon in baseball.
- •
Most core muscle injuries resolve without surgery. Those that require surgery often involve the attachment of the rectus abdominis and hip adductors to the pubic bone.
- •
MRI with athletic pubalgia or Jefferson protocol is useful in defining the muscles involved and the extent of core muscle injuries.
- •
Repetitive hyper-abduction movements (such as pitching) can give rise to scarring in the adductor muscle belly (Baseball Pitcher/Hockey Goalie syndrome) that can occur with or without pubic plate injuries.
Introduction
Anatomy of the Core Muscles
The concept of “the core” was established by exercise and fitness experts and refers to the entire body from the chest to the mid-thigh. This classification allows for further subcategorization based on the anatomic structures involved. Specifically, there are 4 broad categories of core injuries: muscular, hip, back, and everything else.
Understanding core muscle injuries necessitates a focus on the pivotal role of the muscles that anchor to the pubic bone. These muscles are symmetrically arranged around the pubic bone and are central to core stability. This core stability is fundamental in underpinning an athlete’s performance across a broad spectrum of activities.
The group of muscles attaching to the pubic bone, the rectus abdominis, and the hip adductors (the pectineus, adductor longus, and adductor brevis), are essential for maintaining pelvic stability. This stability is not just about preventing injuries; it’s about creating a solid foundation from which all athletic movements can be optimized. These pubic ‘harness’ muscles facilitate a harmonious connection between the upper and lower body, enabling the transfer of power that is essential for peak performance. They are the primary conduit for the transfer of power from the lower extremities to the upper body in both the throwing and swinging motions. It has been established that limited mobility, strength, and endurance at any point in the kinetic chain can impact performance, and the core muscles are as important as any other.
Furthermore, the interplay between these muscles and the stability they provide cannot be overstated. The adductor muscles, for example, are not only crucial for bringing the legs together but also play a significant role in stabilizing the body during movements that require a high degree of balance and coordination.
Research in other sports (primarily soccer) has identified that previous adductor injuries are a significant predictor of subsequent core muscle injuries involving the rectus abdominis, adductors, and hamstrings. Similarly, the authors have found in clinical practice that distal scarring from a muscle belly injury can increase the forces applied at the pubic bone attachment and can accelerate a central injury. Other muscles, such as the iliopsoas and rectus femoris, can be involved as well. In a review of experience with over 8000 patients, these muscles were involved in 3% and 4% of cases, respectively. This highlights the importance of targeted prevention strategies, focusing on strengthening and maintaining the health of these key harness muscles.
It is important to consider the connection between the core musculature and the hip joints. Symptomatic femoroacetabular impingement (FAI) and core muscle injuries have been observed in similar athletic populations and concurrently in the same athlete. In our practice, 16% of patients have symptomatic intra-articular hip pathology in addition to muscular injury. Focusing on high level athletes, Larson and colleagues studied a subset of patients with both symptomatic intra-articular hip pathology and core muscle injuries. Management of the muscle injuries alone led to a 25% return to pre-injury level of play. Treating both the intra- and extra- articular symptoms concurrently led to an 85% return to pre-injury level of play. Treating both sets of problems in a stepwise manner yielded a 93% return to pre-injury level play. Economopoulos and colleagues found radiographic evidence of FAI in 86% of patients who were treated surgically for athletic pubalgia. Birmingham and colleagues suggest an interesting mechanism for this hip-core muscle connection: the presence of Cam impingement was associated with 35% more rotational and transverse motion at the pubic symphysis. In the investigators’ practice, the authors observe increased resting tension in the adductor muscles among patients with symptomatic FAI and increased adductor fibrosis (observed intraoperatively) among those patients.
The muscles attaching to the pubic bone constitute a harness that serves as the bedrock of core stability, underpinning the athleticism that defines performance in sports. A comprehensive understanding of their function and the commonality of injuries in this area is crucial for developing effective interventions aimed at enhancing athletic longevity and minimizing the risk of injury.
Incidence of Core Muscle Injuries in Baseball
Despite increasing recognition, these injuries remain poorly understood compared with other sports injuries. This is likely in part because of the diversity of organ systems that can give rise to lower abdominal or groin pain. Additionally, the lack of consistent nomenclature makes studying them difficult. By using categories based on the locations of pain, the authors do know that injuries of the upper leg, groin, and hip are among the most common injuries in sport. ,
In the investigators’ practice, baseball players (high school, collegiate, and professional) constituted 5.2% of our patient population in 2023. ( unpublished data from the Vincera Institute patient database ) There are numerous studies of baseball athletes that suggest that core muscle injuries are common in the sport. Posner and colleagues identified an increased incidence of core injuries among Major League Baseball (MLB) players from 2002 to 2008, with approximately 43% of injuries involving the core. Coleman and colleagues determined that 5.5% of all injuries in the MLB and minor (MiLB) leagues between 2011 and 2014 involved the hip or groin and 96% of those injuries were extra-articular. With respect to abdominal muscle injuries, Conte, and colleagues reported that these injuries constituted 5% of all injuries in MLB players present on the disabled list between 1991 and 2010. In a survey of baseball related injuries in 100 high schools from 2005 to 2007, chest, rib, and abdominal injuries accounted for 2.1% of the total, while 2% of injuries involved the hip and 7.9% of the thigh.
Mechanism of Injury
There are many position-specific mechanics that can give rise to core muscle injuries. There are also some global considerations within the sport. In general, core muscle injuries develop from repetitive stress that leads to disruption of the attachments of the muscles to the pubic bone in what is typically an acute on chronic injury. Disruptions in athletes’ routine, such as sudden increases in workload because one is being promoted to a new level of competition or when returning from a break because of injury or off season, also seemed to play a role. In this section, the auhtors will go through the mechanics of throwing and batting, and discuss their implications with respect to the core muscles. The authors will then look at some of the positions and discuss factors specific to those roles.
Throwing
Throwing begins with the initiation of movement to create momentum, which for a position player may be a crow hop to get the feet set and for a pitcher on the mound is planting the back foot against the rubber. At the start of the windup, the dominant lower extremity sets into a balanced position of slight hip and knee flexion, with the hip abductors firing to keep the pelvis level. The plant (non-dominant) lower extremity undergoes concentric hip flexion while balance is maintained on the back leg. The gluteal and paraspinal muscles are activated during the wind up to keep the trunk stabilized as it stays relatively perpendicular to the target and the body stays relatively upright. The acceleration phase involves a quick and dramatic weight shift. The obliques join the rectus abdominis to create trunk rotation. External rotation of the plant leg hip leads to forceful abduction of the non-dominant leg as the dominant lower extremity forcefully internally rotates and adducts in coordination with the flexion of the abdomen. The amount of flexion, length of stride, and position of the trunk have huge implications on the force dynamics within the throwing arm and the development of core muscle injury. During the follow-through phase, the abovementioned movements quickly decelerate. The forces shift to the upper extremity and this force transfer is another opportunity for injury.
Batting
The classic cocking, coiling, acceleration, and follow-through phases of batting involve basically the same processes and transfers of forces as throwing. However, because the forces are distributed more widely, repetitive swinging seems to result in fewer injuries compared with pitching. Altered mechanics, as in while compensating for injury or unsure footing, are often in play when core muscle injuries do develop. Batters with core muscle injuries often report difficulty in catching up to fast balls and often are forced to look for off-speed pitches. In addition, many professional hitters with core muscle injuries report the most pain with swings and misses, which highlights the amount of force being transferred across the pubic bone during the swinging motion.
Diagnosis of core muscle injuries
Physical Examination
A comprehensive history and physical examination, and appropriate imaging are necessary to arrive at a complete diagnosis. Localized tenderness may sometimes help for specific diagnoses, although tenderness from diffuse bony or soft tissue inflammation may also cause confusion. Resistance testing with careful attention to the location of elicited pain can help identify involved muscles. Interpretation of each test involves 3 considerations: Does the test cause pain? Does the resulting pain correlate to the muscle being tested? And does the resulting pain recreate the pain causing the athletes disability? One must also consider that portions of the gastrointestinal, genitourinary, and gynecologic systems; lymphatics, blood vessels, and nerves also reside in the core. The importance of this group cannot be overstated because some of these diagnoses can be life threatening. A detailed history and physical examination will often provide enough evidence to expand the focus beyond the musculoskeletal system.
Diagnostic Imaging
Because ultrasound is relatively inexpensive and widely available, it is often an appropriate next step. The presence of edema around the pubic bone or along the surrounding musculature, or signs of atrophy or laxity of the abdominal wall should prompt one to get an MRI with the “athletic pubalgia” or Jefferson protocol to better define the muscles involved.
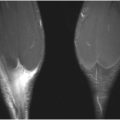
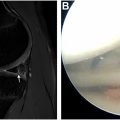
The authors place primary importance on the presence of fluid between the pubic bone and the overlying fibrocartilage plate ( Fig. 1 ). The presence of peri-pubic and bone marrow edema (osteitis pubis) is a secondary sign of injury and it should raise one’s suspicion for a plate detachment. It is important to recognize that in skeletally immature patients, the fluid can be present along the growth plate (ie, subphyseal, Fig. 2 ). This has been referred to as a “secondary cleft” and can easily be overlooked. Chronic plate detachments ( Fig. 3 ) can also be more difficult, occurring in long-standing injuries where spicules of granulation tissue fill in portions of the gap between the fibrocartilage plate and pubic bone. Degenerative plate detachments have a similar appearance but the edges of the fibrocartilage develop a lytic appearance, and the authors think these occur with repetitive trauma ( Fig. 4 ). It is also important to keep in mind that conventional Mendelian randomisation (MR) studies of the pelvis or hip are often read as normal ( Fig. 5 ) or as showing some nonspecific changes of the pubic symphysis or edema patterns, leading to incorrect diagnoses, such as stress fracture or even worse, no injury.