Zones of adherence that should be avoided during contouring of the lower extremities
It is the author’s preference to perform VASER-assisted liposuction (VAL) for body contouring procedures including harvesting for gluteal fat grafting. The VAL procedure is far less traumatic than traditional liposuction (SAL); yields highly aesthetic, precise, results; and has minimal associated complications [7, 8]. In addition, the author has reported significantly less blood loss in the aspirate of a large series of VAL patients following contouring of the posterior trunk when compared to SAL patients who underwent contouring of similar areas [9, 10]. When used at the clinically recommended settings, VASER aspirate is an emulsion of live adipocytes. The adipocyte viability in VASER aspirate has been confirmed by several studies [11, 12]. It is the author’s opinion that scanning electron microscopy of the aspirate specimen is far more accurate than simple viability stains in assessing the quality of a fat harvest. Adipocytes exposed to higher levels of ultrasound energy can display altered morphology under electron microscopy evaluation but can still stain as viable under certain conditions [13]. In these instances the aspirate may contain viable adipocytes but morphological alterations present may render them unsuitable for fat grafting. Electron microscopy studies of VASER aspirate, acquired under clinically recommended energy settings and exposure times, display normal, unaltered morphology of well-separated adipocytes [14]. VASER aspirate acquired under these conditions serves as a highly suitable harvest source for fat grafting.
Preoperative Considerations
In regard to gluteal contouring, it is imperative that both the patient and the surgeon are well aligned in respect to the aesthetic goals of the operation. Is the patient seeking a rounder, more athletic buttock shape or just simply a bigger butt? Sculpting a round, athletic buttock shape typically does not require adding volume. Fat grafting may be required in some cases where the contouring alone is not enough to correct a visual gluteal deficiency, but in the author’s experience with these cases, the grafted volumes are small to moderate and seldom exceed 500 ml per buttock injected into the subcutaneous plane. In recent years there has been a significant increase in the volumes grafted by some surgeons during these procedures. It was not unusual for surgeons to graft over 1000 ml of fat per buttock and occasionally the volumes grafted were as high as 1500 per buttock! These massive volumes required grafting into the gluteal muscles which significantly increased the surgical complications. Patient deaths as a result of fat emboli continued to rise [15], until gluteal fat grafting was associated with the highest mortality rate of any aesthetic surgical procedure.
For safety reasons, gluteal enhancement by means of fat grafting has recently become an operation of the subcutaneous tissues. As plastic surgeons move away from intramuscular grafting, the volumes grafted will need to be adjusted accordingly. Tissue compliance and overall gluteal surface area will play a significant role in determining the fat graft volume limits for a particular patient, in order to not exceed the recipient site capacity. Since subcutaneous grafting has obvious volume limitations, creating the visual of a voluminous buttock will require more aggressive contouring of the surrounding areas.
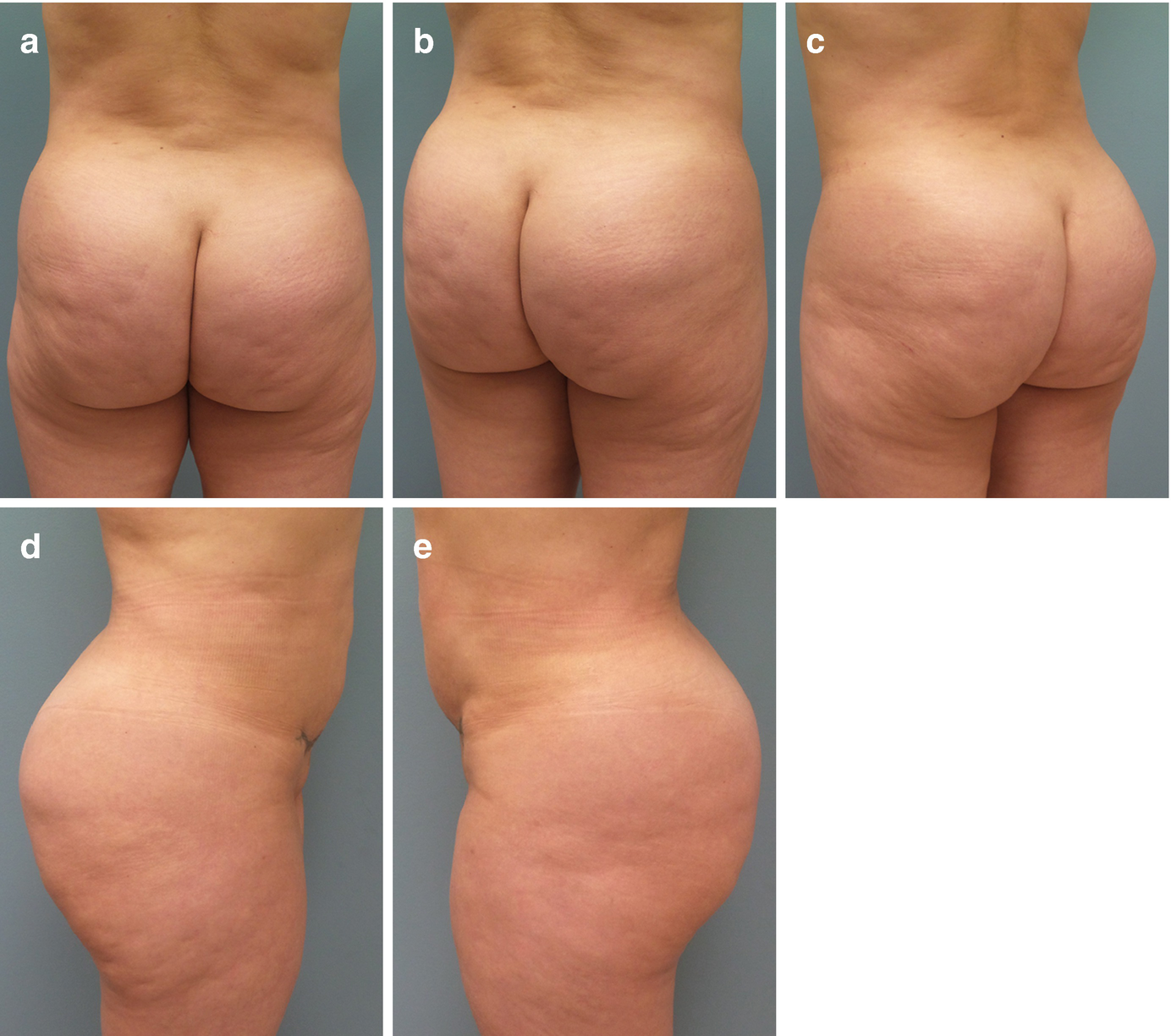
Preoperative photography for gluteal contouring includes posterior, right/left oblique, and right/left lateral views. (a) posterior, (b) right oblique, (c) left oblique, (d) right lateral, (e) left lateral

A complete posterior view of the back is suggested in female patients to evaluate waistline contour

Preoperative markings for gluteal contouring
Surgical Technique
Gluteal contouring with or without fat grafting requires aggressive fat extraction from the posterior flanks. Lipodystrophy of the saddlebags and infra-gluteal areas also needs to be addressed by the extraction. As opposed to males where aggressive contouring of the waist provides the desired aesthetic results (small waist/wide back), aggressive sculpting of the waistline on female patients requires extending the contouring into the upper back in order to avoid a masculine appearance postoperatively (small waist/wide back).
Positioning is somewhat controversial since some authors recommend the prone position for contouring the posterior flanks and back while others prefer the lateral decubitus position. The prone position is more convenient since it only requires that the patient be repositioned twice on the operating table (supine-prone-supine). Also, this position allows for visual assessment of both sides simultaneously. The lateral decubitus position requires that the patient be repositioned three times on the operating table (supine-right lateral decubitus-left lateral decubitus-supine). In spite of the slightly longer surgical times associated with the lateral decubitus positions, this author as well as other experienced body contouring surgeons frequently use the lateral decubitus positioning when contouring the waistline [16, 17]. The posterior triangle, an important component of the aesthetic waistline, cannot be adequately addressed from the prone position.
Since these cases generally involve contouring of fairly large surface areas, they are performed under general anesthesia and typically as an outpatient procedure. The lateral decubitus position requires padding of pressure points and an axillary roll. A Bean Bag Surgical Positioner (Medline Industries, Northfield, IL) is helpful in maintaining the desired patient position on the operating table. A Bair Hugger (3M, St. Paul, MN) is placed over the non-operative areas and the intravenous fluids are warmed. A Foley catheter is commonly used to monitor urine output in cases where high volumes of wetting solution are employed. The rationale behind the wetting solution formula has been discussed in detail elsewhere in this textbook (Chap. 4). For general anesthesia cases, the author employs a formula consisting of 1 ml of epinephrine 1:1000 in a liter of Ringer’s Lactate solution at room temperature. Ultrasound to the posterior trunk is delivered by a 3.7 mm, 2-ring VASER probe (Solta Medical, Bothell, WA) at 80% in pulsed mode. Aspiration is performed with 4.6 mm, 3.7 mm, and 3.0 mm VentX cannulas (Solta Medical, Bothell, WA). Postoperatively, TopiFoam (Mentor Corp., Irvine, CA) and compression garments are utilized.
Surgical Outcomes

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


