Continuous Wave Doppler
 WHEN TO PERFORM A DOPPLER EXAMINATION
WHEN TO PERFORM A DOPPLER EXAMINATION
When there is a need to supplement the physical examination, continuous wave Doppler (CWD) was the test modality most often available to the clinician until compact, affordable Duplex units became readily available. The CWD examination was considered as an essential part of every physical examination of the venous system and the handheld Doppler was considered to be the “stethoscope” of the phlebologist. Although largely replaced by Duplex ultrasound, a basic understanding of use of the stethoscope of phlebology is still important.
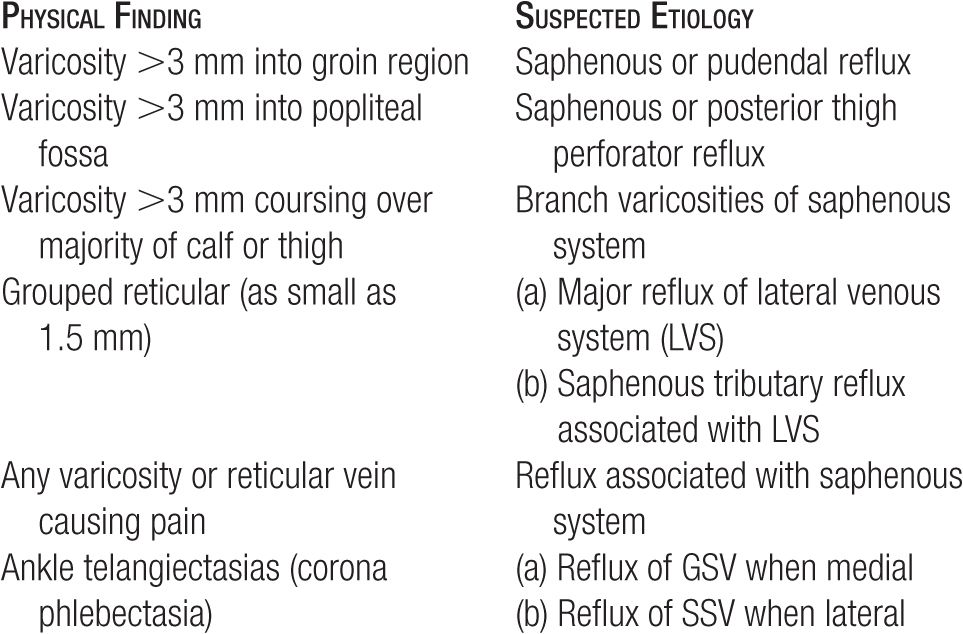
Continuous wave Doppler or Duplex ultrasound can provide essential information in many clinical presentations: when a patient complains of pain related to varicosities, when the physical examination reveals varicosities larger than 3 mm in diameter, when varicosities of any size extend into the groin or the popliteal fossa, and when a feeding vessel is sought for a focal area of grouped venulectases (1–2 mm).1 Guidelines for the use of this diagnostic aid to physical examination are listed in Table 8-1. Doppler examination may suggest the need for additional testing but is especially helpful as an inexpensive screening tool if a duplex ultrasound examination is not available as is currently the case in many developing nations.
TABLE 8-1
Guidelines for the use of Doppler
The purposes of the CWD examination are multiple: to identify or rule out reflux at the saphenofemoral and saphenopopliteal junctions, to trace the course of varicosities, and to identify other points of reflux through incompetent perforating veins in the thigh, calf, and ankle (Table 8-2). CWD also gives an approximate sense of the speed and phasicity of venous flow at the saphenofemoral junction.
TABLE 8-2
Purpose of CWD Doppler Examination (mainly replaced by Duplex ultrasound)
Identify or rule out reflux at the saphenofemoral and saphenopopliteal junctions
Identify most proximal point of reflux through branches off the saphenous system
Trace course of varicosities
Identify other points of reflux through incompetent perforating veins in the thigh, calf, and ankle
Many physicians are familiar with the rapid, pulsatile sound of CWD as used for the detection of fetal heart sounds and faint arterial sounds. In general, higher velocities of flow produce higher-pitched Doppler sounds and higher volumes of flow produce louder sounds. Venous flow produces a nonpulsatile, fairly low-pitched, ghostly blowing sound (“wind in the rigging”) that is often heard as a background to arterial sounds.
 PRINCIPLES OF DOPPLER ULTRASOUND
PRINCIPLES OF DOPPLER ULTRASOUND
Doppler ultrasound is named after the famed Austrian physicist Johann Christian Doppler, who in 1842 explained an apparent increase or decrease in the frequency of waves emitted or reflected from an object that is moving toward or away from the observer. The essence of the principle is this: when the object is moving toward the observer, each wave is emitted or reflected from a position a little closer than the one before; thus, each wave comes back a little sooner than expected and the frequency appears to be higher. When the object is moving away from the observer, each wave comes back a little later than it would if the object was not moving, so the frequency appears to be lower.
The Doppler principle applies to all types of wave phenomena in all types of media. Doppler is still an essential component of the Duplex ultrasound examination. The principle is familiar for its use in radar speed detection: when a radar gun is pointed at a stationary object, the reflected (returning) radar waves have the same wavelength and frequency as the emitted (outgoing) waves, but when the signal is reflected from a moving object (such as a car), the reflected waves have a wavelength and frequency that are different from those of the emitted waves. If the car is moving away from the radar gun, the reflected waves are farther apart than the emitted waves. If the car is moving toward the radar gun, the reflected waves are closer together than the emitted waves.
Doppler ultrasound probes use piezoelectric crystals to emit high-frequency (ultrasound) waves and to detect reflected waves returning to the probe. Ultrasound waves are reflected from many structures, but all the waves that return with the same frequency are ignored. When sound waves are reflected from blood cells that are moving relative to the probe, the frequency of the emitted waves is compared with that of the reflected waves, and the difference between the two (the Doppler shift) is an indication of the speed and direction of flow (Figure 8-1).
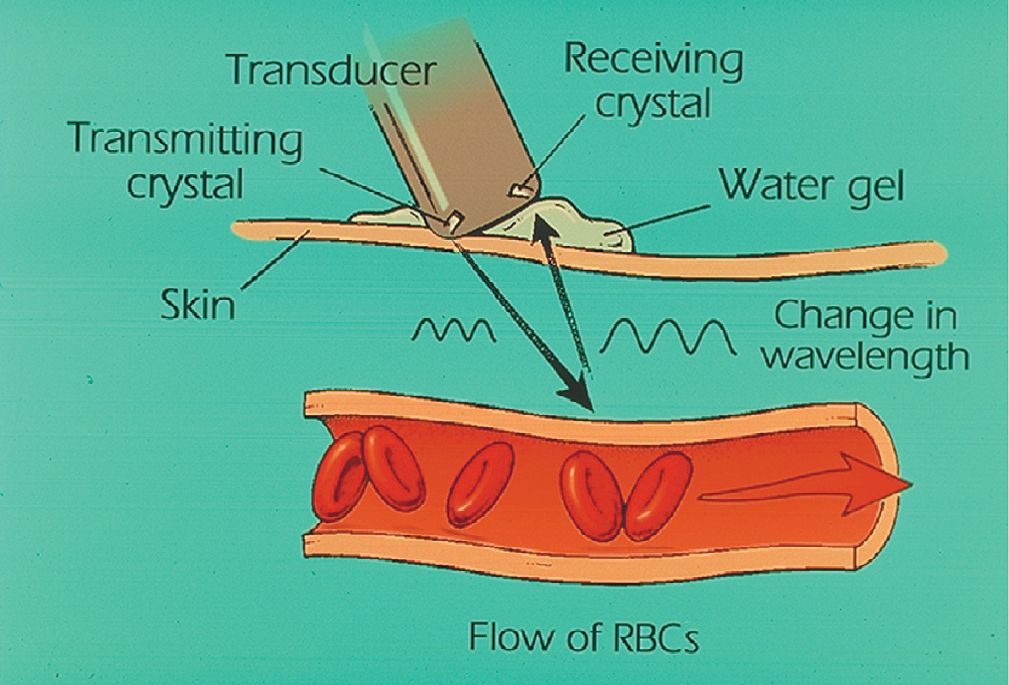
![]() FIGURE 8-1 Schematic of Doppler ultrasound operation. The application of water-based gel allows a continuous medium for transmission of ultrasound. Red blood cells flowing away from the probe cause a decreased frequency reflected to the receiving crystal. This frequency shift is detected by the receiving crystal and causes an audible sound.
FIGURE 8-1 Schematic of Doppler ultrasound operation. The application of water-based gel allows a continuous medium for transmission of ultrasound. Red blood cells flowing away from the probe cause a decreased frequency reflected to the receiving crystal. This frequency shift is detected by the receiving crystal and causes an audible sound.
Handheld Doppler units use the Doppler shift frequency to modulate an audible sound that is lowest in pitch when there is slow flow and highest in pitch when there is high flow. The volume of a pitch depends on the number of cells flowing at a given velocity. The sound produced by a Doppler unit is a mixture of many different sound frequencies because not all of the blood cells flow through the vessel at the same speed. Turbulence causes abrupt variations in flow velocity and direction, while friction produces a smooth gradient of velocity from the slowest-moving layers of fluid adjacent to the vessel walls to the fastest-moving layers in the middle of the stream. Each point of signal reflection makes a separate contribution to the aggregate sound reflecting the overall flow conditions within the vessel.
Many units can also produce a printed tracing of the speed, direction, and relative amount of flow. Unidirectional Doppler measures the speed of flow relative to the probe without considering the direction, while bidirectional graphing Doppler can identify movement as being either toward or away from the transducer. Bidirectional Doppler is primarily used for waveform analysis of arterial pulses and is less useful for the analysis of venous reflux. In the venous system, the timing of flow sounds relative to various maneuvers that are performed best assesses the direction of flow.2 Phlebologists have come to prefer bidirectional Doppler in recent years principally because most third-party payors will reimburse a patient for Doppler examination only if there is a printed bidirectional tracing.
Doppler probes of different frequencies are used depending on the depth of the vessels to be examined because lower frequency ultrasound penetrates deeper through tissues before being reflected back to the transducer. A Doppler probe that emits frequencies of 8–10 MHz is best suited to examining vessels that are less than 2 cm deep, although we find it difficult to hear reflux greater than 1 cm below the skin surface with these frequencies. Vessels up to 4 cm in depth may be examined using a 5-MHz probe.3
To prevent signal loss, a coupling gel must be applied between the skin and the Doppler probe to eliminate any air between the two surfaces. Good results will only be obtained with a liberal amount of gel and a very light touch where the probe makes contact with the skin. The Doppler probe angle is also very important in obtaining a good-quality signal: the Doppler effect detects only movement toward or away from the probe, so if the Doppler probe is at right angles to a vessel, there will be no net Doppler shift of the reflected signal, and thus no flow will be detected. A probe angle of 45° relative to the vessel gives the most consistent signal with the least variation due to changes in the direction of unseen vessels.4
Continuous Wave Doppler Ultrasound in Phlebology
Although Doppler ultrasound is useful in the assessment of any condition in which arterial or venous flow dynamics are altered, the primary phlebological purpose of venous Doppler ultrasound examination is the detection of retrograde venous flow (venous reflux) due to absent or malfunctioning venous valves.
To use CWD for venous diagnosis, one must be familiar with a standard examination and with the usual findings in a normal patient. Under normal conditions, spontaneous and respirophasic forward (cephalad) flow may be recorded in the common femoral vein, at the saphenofemoral junction, and occasionally at the popliteal vein. Doppler ultrasound is relatively insensitive to slow flow; thus, detection of forward flow in other veins usually requires manual augmentation (squeezing the distal extremity in order to increase the volume and velocity of antegrade flow at the point of auscultation).
Abnormal spontaneous flow is detectable in areas of stenosis, where the normal flow velocity speeds up as it passes through the narrowed channel. Abnormal spontaneous flow may also be heard in any vein when the legs are extremely congested due to significant venous reflux. Retrograde venous flow is always abnormal: the detection of more than a half second of retrograde flow at any level always indicates incompetence of the valves in the vein being examined, whether the retrograde flow occurs spontaneously, upon Valsalva, or with reverse augmentation (Figure 8-2).
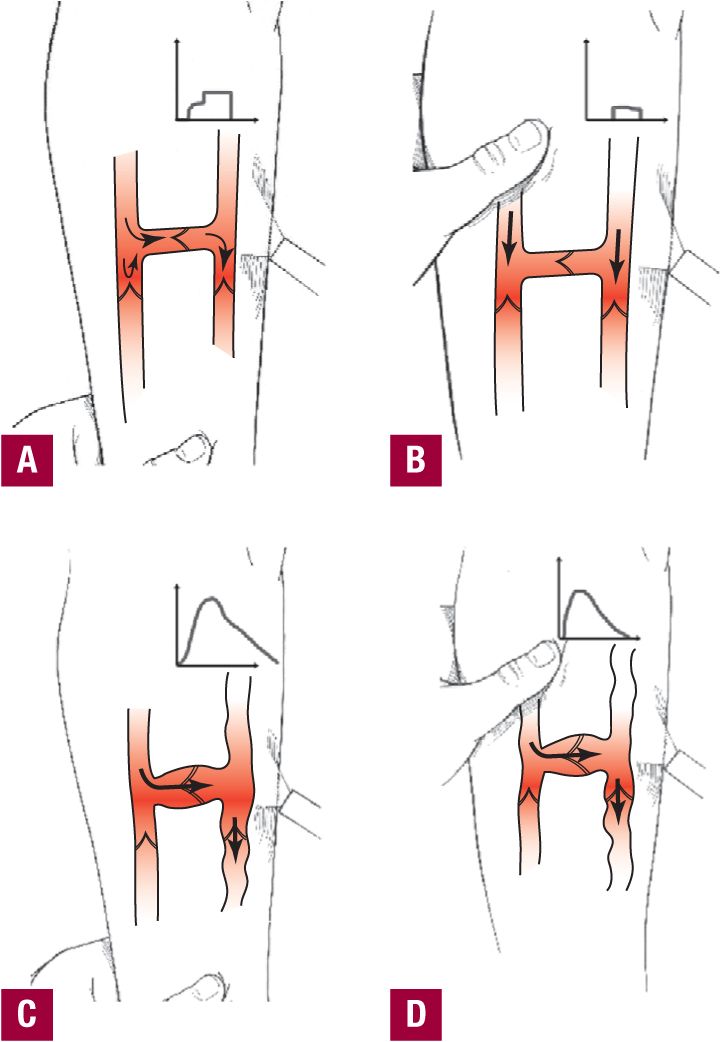
![]() FIGURE 8-2 Proximal and distal compression by Doppler ultrasound examination. Competent Perforator Valve. A. During distal compression, brief normal forward flow is heard (inset). As distal compression is released, blood flows backward under gravity but is rapidly stopped by competent valves. B. During proximal compression, a brief sound is heard (inset), which rapidly concludes as blood movement is stopped by competent valves. Incompetent Perforator Valves. C. During distal compression, a brief normal upward flow is heard; however, as distal compression is released, blood flow continues backward with a prolonged sound (inset), as incompetent valves are unable to prevent continued flow propelled by hydrostatic pressure (gravity). This is the most reliable way to measure for reflux. D.
FIGURE 8-2 Proximal and distal compression by Doppler ultrasound examination. Competent Perforator Valve. A. During distal compression, brief normal forward flow is heard (inset). As distal compression is released, blood flows backward under gravity but is rapidly stopped by competent valves. B. During proximal compression, a brief sound is heard (inset), which rapidly concludes as blood movement is stopped by competent valves. Incompetent Perforator Valves. C. During distal compression, a brief normal upward flow is heard; however, as distal compression is released, blood flow continues backward with a prolonged sound (inset), as incompetent valves are unable to prevent continued flow propelled by hydrostatic pressure (gravity). This is the most reliable way to measure for reflux. D.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


