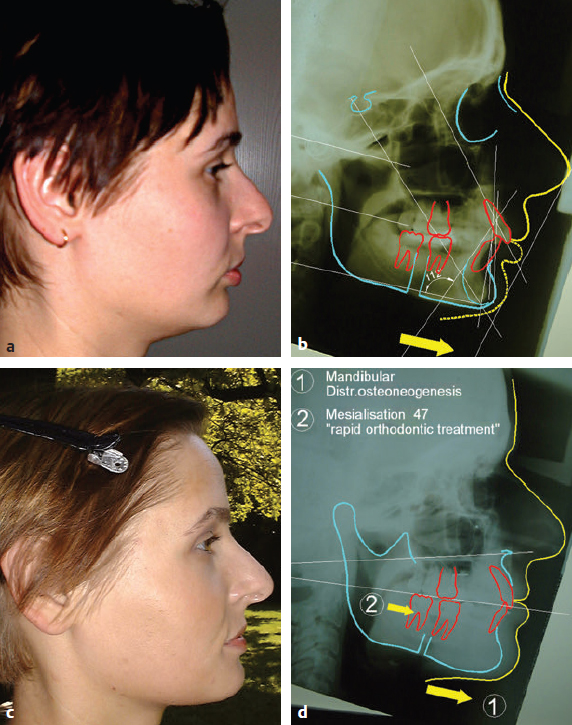
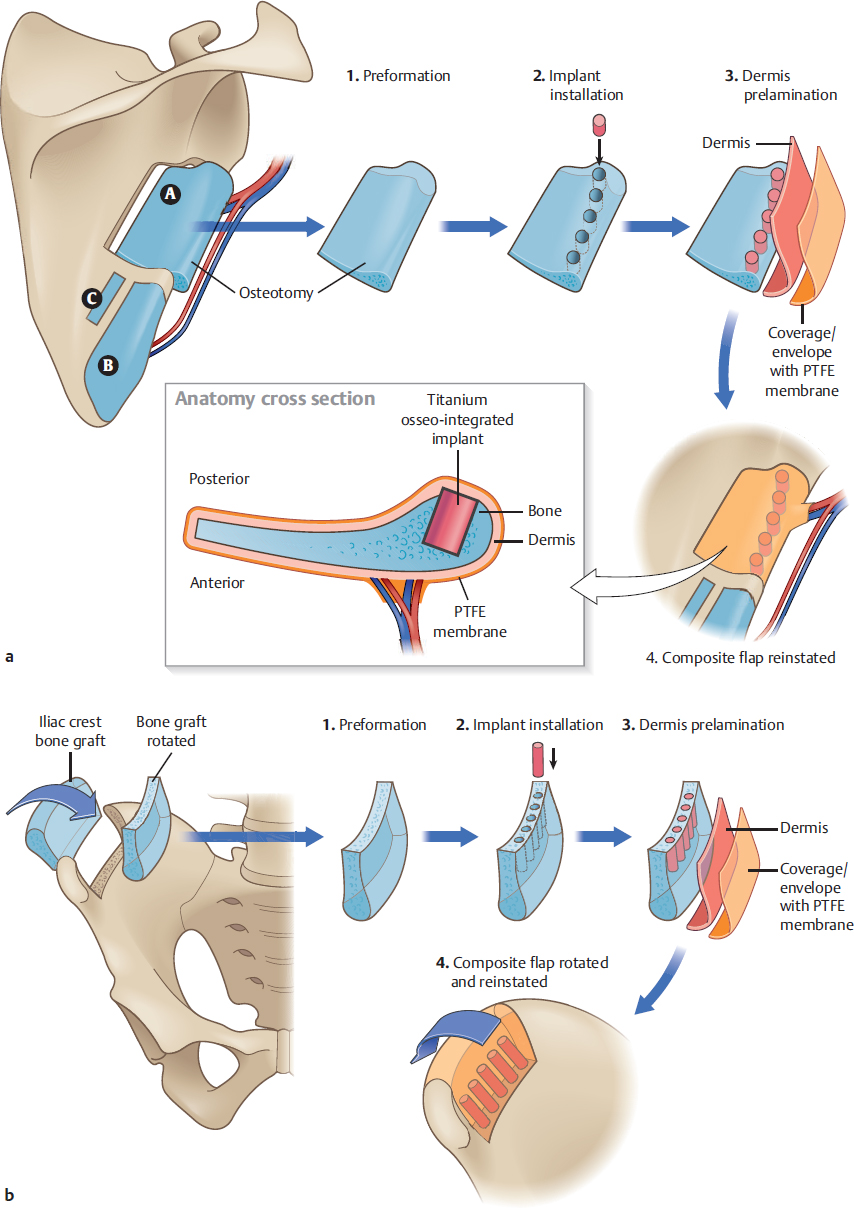
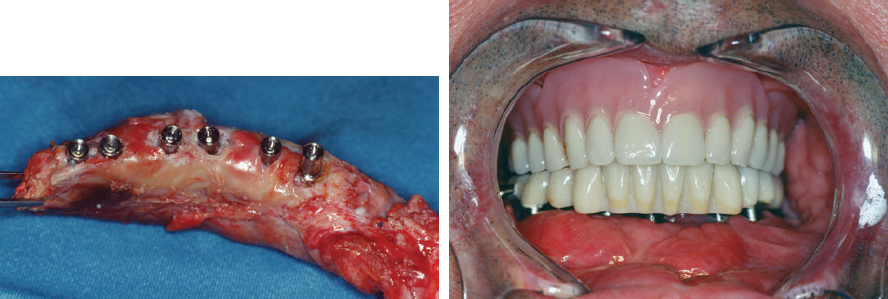
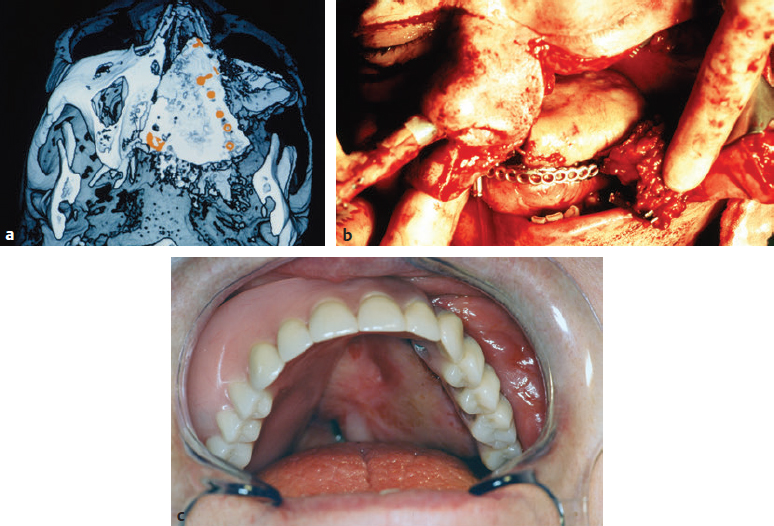
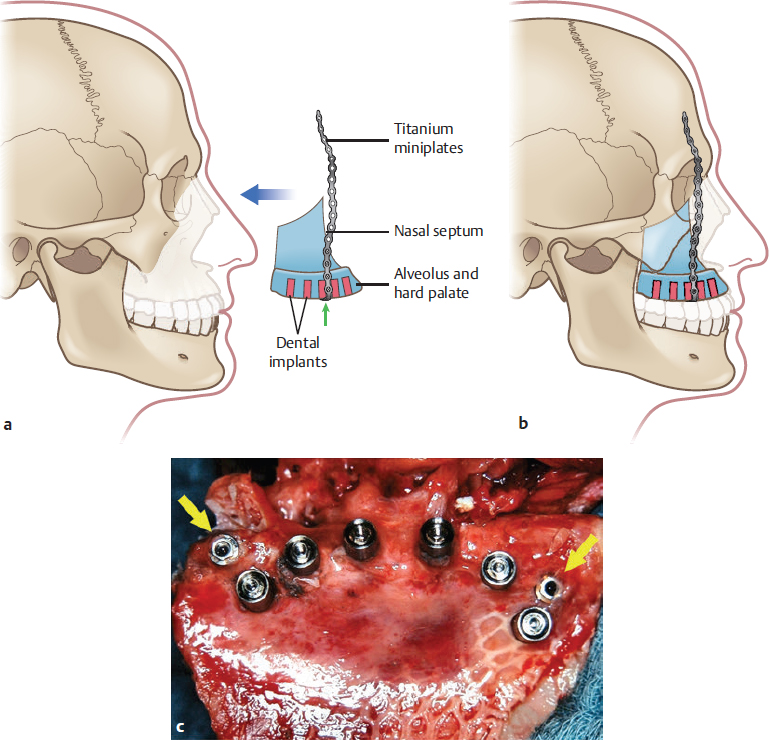
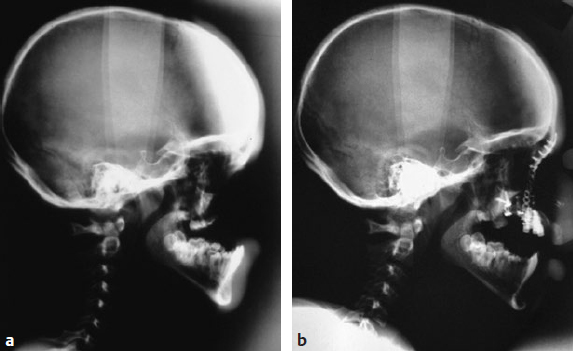
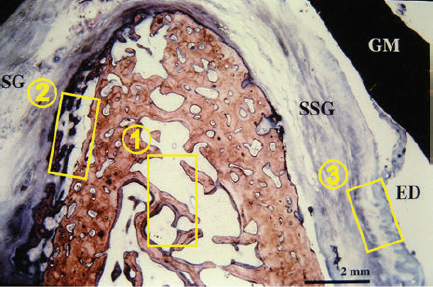
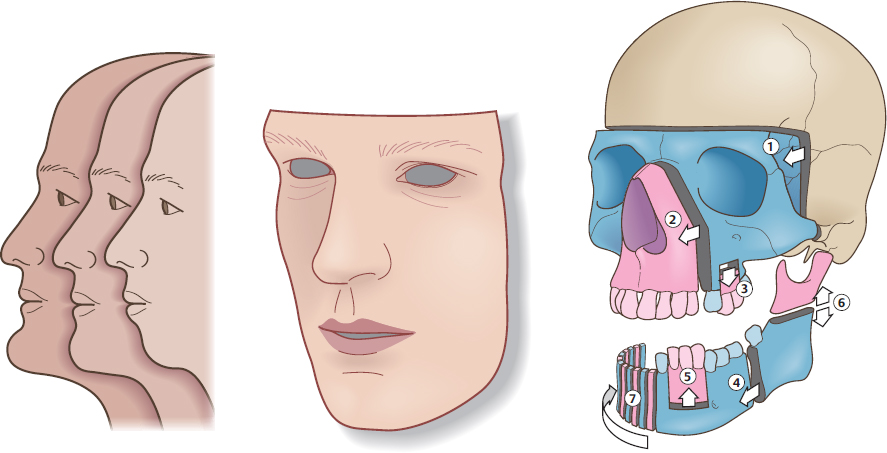
CHAPTER Modern plastic surgery concepts are based on the paradigm that plastic surgery must restore function as well as anatomy in all cases, regardless of the indication for surgery. In the case of facial plastic surgery, respecting the facial proportions is an elementary prerequisite for achieving an aesthetic reconstruction.1 The facial skeleton is a lightweight, mechanically stable structure that contains pneumatized cavities, houses organ systems, and allows for the fixation of the facial soft tissue envelope in a way that maintains musculoskeletal balance. In the case of loss or aplasia of facial parts, facial disfigurement increases in parallel with the extent of the maxillofacial defect. In this situation, ignoring the functional anatomy during the reconstruction effort invariably results in unsatisfactory outcomes. Since the introduction of microsurgical flap transfer, other methods of regenerative plastic surgery involving the induction of bone and soft tissues in surgical protocols with advanced block-grafting techniques, including prefabricated composite grafts and distraction osteogenesis and histogenesis, have been introduced and can help avoid unfavorable results in patients with severe maxillofacial defects. The bone–muscle crosstalk, which is associated with the regenerative plastic surgery methods mentioned earlier, has beneficial clinical effects on the musculoskeletal balance of the face and is useful for achieving a full rehabilitation. Restorative plastic surgery requires the simultaneous reconstruction of maxillofacial aesthetics and function in all cases, regardless of the indication for surgery, and relies on the surgical concept of like-with-like reconstruction combined with the skeletal rearrangement of the disfigured face. By considering aesthetics and function as an inseparable unit during the induction of functional tissues, the historical separation between plastic reconstructive and aesthetic surgery has been broken. Summary Box Complications in Maxillofacial Reconstruction • Absence of physiologic mucosal lining and gingiva • Facial deformity • Need for repeat bone grafts • Oral mobility loss • Implant loss • Excessive mucous secretion • Persistent peristalsis • Maceration • Hair growth The face is involved in speaking, mastication, deglutition, and effortless breathing, and these functions dictate the main objective of any facial treatment: to restore physiological function. The reconstruction of the face, a pneumatized, lightweight, mechanically stable structure to which the facial soft tissue envelope is fixed to maintain musculoskeletal balance, has proven to be a surgical challenge. Fig. 50.1 (a) An unfavorable result caused by intraoral bulkiness in a 58-year-old woman after hemimaxillectomy and reconstruction with an osseomyocutaneous flap. (b) An unfavorable result caused by extraoral “sinus bulkiness” in a 27-year-old patient with loss of the maxilla after tumor surgery and postoperative radiotherapy. Combination of prefabricated scapular flap and obturation of the sinus with a teres major flap. (c) An unfavorable result caused by “bony bulkiness” in a 57-year-old patient after microsurgical reconstruction of the mandible, tongue, and mouth floor with an iliac prefabricated composite graft and external oblique muscle free flap, first described in 1997. (a From Zimpfer M. Department of Anesthesiology and General Intensive Care University of Vienna 1996–2000 Patient Care–Teaching–Research, self-published; b,c from Holle J, Vinzenz K, Würinger E, Kulenkampff KJ, Saidi M. The prefabricated combined scapula flap for bony and soft-tissue reconstruction in maxillofacial defects—a new method. Plast Reconstr Surg 1996;98(3):542–552.) Among the established core principles of craniofacial surgery including “safe approaches, careful designed osteotomies and rigid skeletal fixation”2; advanced bone grafting techniques using the induction of specialized hard and soft tissues in the reconstruction effort are part of the trendsetting advances in regenerative plastic surgery.2 Vascularized osseous, osseocutaneous and myocutaneous free flaps, preferably taken from the fibula, scapula or iliac crest, are standard techniques in facial plastic surgery today.3 The techniques of soft tissue flaps and the microsurgical revascularization of transplants in the maxillofacial area, on the other hand, have not changed significantly since their introduction and are not discussed further here. From a functional point of view, the shortcomings of the use of the current standard free flap methods in facial plastic surgery are as follows: • Closure in severe defects with myocutaneous flaps, irrespective of dermal texture4 • Obturation of pneumatized cavities6 • Reconstruction of a bony framework rather than restoration of the anatomy7 In addition, the current free flap methods occasionally result in bulkiness, which prevents the satisfactory restoration of aesthetics and function5–7 (Fig. 50.1). Stepwise adaptations and corrections can help to achieve acceptable clinical outcomes, but only in the case of mandibular reconstructions6 (Fig. 50.2). Fig. 50.2 Stepwise aesthetic and functional rehabilitation by trimming bulky flaps and integrating implant restoration. (From Holle J, Vinzenz K, Würinger E, Kulenkampff KJ, Saidi M. The prefabricated combined scapula flap for bony and soft-tissue reconstruction in maxillofacial defects—a new method. Plast Reconstr 1996;98(3):542-552.) For the reconstruction of a pneumatized midface, these free flap techniques are inappropriate, which has led to the trend of patient-specific implants and full-face transplantation.8–10 There is a flowing transition between tissue deficiency and defect, and if these persist long enough, they are usually combined with facial disfigurement; therefore complex surgical protocols, rather than simple free flap techniques, are necessary to avoid unfavorable results. The surgical concept of like-with-like restoration in the case of the oral and maxillofacial anatomy includes both the reconstruction of missing tissues and the rearrangement of the skeletal architecture of the face to achieve acceptable aesthetic and functional results, which can be best illustrated in cleft patients. Two aspects must be taken into account during the treatment of maxillofacial deficiencies or defects: 1. Like-with-like reconstruction based on the three “identities,” namely, identical size, identical shape, and identical tissue structure to those of the recipient site.6,11,12 2. Correction of facial disfigurement using grafts and/or surgical orthognathic procedures.13,14 Depending on the extent of the tissue deficiency, a series of surgical methods have been described for different indications in maxillofacial surgery: • Osteoplastic reconstruction (e.g., “stack plasty”) of the alveolus and osteoplasty of tertiary clefts14 • Prefabrication and prelamination of osseous grafts for the reconstruction of large alveolar defects15 • Complex prefabricated grafts for microsurgical reconstruction of the maxilla and midface6,12,16,17 From the point of view of functional anatomy, there are four problems that need to be overcome: 1. Reconstruction of a pneumatized, lightweight skeletal structure with mechanical stability 2. Establishment of a stable inner lining of cavities 3. Establishment of gingiva that is resistant to masticatory loading 4. Prevention of graft inflammation, especially at the implant site Before the development of prefabricated composite grafts, the inner lining of the oral cavity was reconstructed using full- or split-thickness skin grafts, intestinal grafts, and mucosal grafts.4,18,19 However, hair growth, maceration, persistent peristalsis, and excessive mucous secretion have diminished the acceptability of these grafts for the replacement of the oral lining. Furthermore, a high rate of implant loss was observed with these grafts because of deep and persistently inflamed pockets around the site where the dental implant penetrated the gingiva. Moreover, attempts at reconstruction with mucosal prelamination of fasciocutaneous flaps failed because of severe scarring of the lining combined with further loss of oral mobility, particularly in the case of reconstructions of the floor of the mouth.18 Fig. 50.3 The surgical procedure for prefabricating composite flaps from the scapula (a) and iliac crest (b). PTFE, Polytetrafluoroethylene. Fig. 50.4 Reconstruction of the mandible with a prefabricated iliac composite graft with a periodontal unit consisting of the bony alveolus, gingiva, and implant restoration in a 57-year-old man who had undergone mandibulectomy. (Reproduced from Vinzenz K, Schaudy C. Osteoplastic surgery of the face—state of the art and future aspects. Eur Surg 2011;43(5):270-283, with permission from Springer-Verlag Wien.) Dermal prelamination of the bone, which was first cited in 1996,6,12 is a complex prefabricated composite graft that allows the restoration of the pneumatized, lightweight skeletal architecture of the face by replacing like with like.6,12,16 As illustrated in Fig. 50.3, the prefabrication of complex composite grafts includes the following: • Preformation of the bony graft • Dermal prelamination of the bony graft • Installation of dental implants The transplant is enveloped in an expanded polytetrafluoroethylene (ePTFE) membrane and allowed to mature at the donor site for several months. After maturation, a graft with a “perfect fit” can be harvested and used for reconstruction. Prefabricated grafts from the scapula are best suited to midface reconstructions, whereas those from the iliac crest are best suited to mandibular reconstructions (see Fig. 50.3) Revascularization is only required for transplants exceeding 4 cm in diameter (Video 50.1).20 A prerequisite for the use of prefabricated grafts is concept surgery, which is defined as surgery that follows a predefined objective and a detailed, preoperatively prepared, stepwise plan, as opposed to routine surgery, which does not involve or strictly follow such plans and may involve a wide variety of perioperative protocols with unknown effects on the surgical outcome.21 Concept surgery requires12,22,23: • A clear definition of the aspired clinical result • Computer-assisted operation planning to transform the surgical concept into clinical reality • Accurate postoperative control using computer-assisted design systems • Critical scientific analysis of the clinical results If these criteria are not met or if a multistage surgery is required at the recipient site, the clinical effort of transplant prefabrication and the physical as well as psychological stress to the patient are difficult to justify.18,24–28 Most of the cited surgical protocols for graft prefabrication have been abandoned because of unfavorable results and complications. Essential in orofacial reconstruction is the prefabrication of an artificial periodontal unit, consisting of the alveolar bone, gingiva, and dental implants, as an integrated component of the entire graft (Fig. 50.4). Thus full oral function is available immediately after the completion of dental restoration.13 Only by inflammation-free periointegration of the dental implants will the implant site be sealed against the oral environment, allowing a stable and successful long-term result.22,23,29 While the alveolar crest of the maxilla can be restored using block-graft techniques,14,15 the pneumatized skeletal anatomy of the midface should preferably be reconstructed using prefabricated composite grafts6 (Fig. 50.5). Midface defects affect all tissue structures and require treatment before disfigurement is caused by the tendency of the tissues to close the defects by shrinking. Fig. 50.5 (a) Three-dimensional computed tomography after surgery to verify the correct fit of a prefabricated composite graft. Note in particular the exact intersection at the palate. (b) Reconstruction of the maxillary sinus as a pneumatized paranasal cavity. (c) Reconstruction of the alveolus and palate in the second quadrant with an attached masticatory gingiva and integrated implant restoration at 6 weeks postoperatively. (From Holle J, Vinzenz K, Würinger E, Kulenkampff KJ, Saidi M. The prefabricated combined scapula flap for bony and soft-tissue reconstruction in maxillofacial defects—a new method. Plast Reconstr Surg 1996;98(3):542–552.) Furthermore, the graft must fit perfectly into the defect (“click in place”), which can be achieved using accurate preoperative computer-assisted planning.12,13,16,17 In complex midface reconstruction, the prefabricated graft is “suspended” into the defect using osteosynthesis titanium miniplates connected to already-osseointegrated dental implants17 (Figs. 50.6 and 50.7) This new method ensures fast restoration of oral function, pneumatized nasal and paranasal cavities, and high graft stability for several years. Therefore this method is preferred in diseases with severe scarring, such as noma.17 Regenerative medicine is the “process of replacing, engineering or regenerating human cells, tissues or organs to restore or establish normal function via stimulating the body’s own repair mechanisms.”30 McCarthy et al,31 who established distraction osteogenesis in maxillofacial surgery before the turn of the millennium, were the first to take craniofacial surgery out of the field of soft tissue and bony reconstructions and into that of tissue engineering and “inductive surgery.” Shortly thereafter, the first scientific studies on tissue induction in prefabricated composite grafts were published.22,23 The main novelty of this procedure is the placement of a dermal graft over the bone to create a substitute for the oral mucosa and avoid the unfavorable results obtained with skin and intestinal grafts. A stable attachment to the bone is essential for the restoration of the inner oral lining (Fig. 50.8). Histomorphologic evaluation of prefabricated composite grafts has shown that the dermis is attached in a periosteum-like manner to the extensively remodeled bone, which osseointegrates the inserted titanium implants, and that the basal parts of the dermis are attached to a papillary connective tissue layer.12 Fig. 50.6 (a–c) An osteosynthesis plate is attached to additional dental implants (yellow arrows) in the graft, and the graft is suspended in the defect (clicked in place). (c From Vinzenz K, Holle J, Würinger E. Reconstruction of the maxilla with prefabricated scapular flaps in noma patients. Plast Reconstr Surg 2008;121(6):1964–1973.) Fig. 50.7 Lateral radiographic studies before (a) and after (b) reconstruction of the entire midface, including the maxilla, palate, and nose, in a patient with severe noma. (From Vinzenz K, Holle J, Würinger E. Reconstruction of the maxilla with prefabricated scapular flaps in noma patients. Plast Reconstr Surg 2008;121(6):1964–1973.) Fig. 50.8 Characteristics of a prefabricated composite graft. (1) Remodeling activity of the bone. (2) An osseomucosal unit with periosteum-like attachment of the lining. (3) Epithelium fixed to the underlying connective tissue by rete ridges. (Reproduced from Vinzenz K, Schaudy C. Osteoplastic surgery of the face–state of the art and future aspects. Eur Surg 2011;43(5):270–283, with permission from Springer-Verlag Wien.) The quality of the epithelium of the inducted bone and the attached lining can be ascertained via immunohistochemical analysis. Most importantly, the prefabricated grafts are covered by an almost normal epithelium within 4 weeks after flap transfer. The epithelium is fixed to the underlining connective tissue by rete ridges. The observation of keratin expression by the epithelial cells indicates a clinically verified complete restitution of the mucosa.23 Because a prefabricated composite graft consists of bone and dental implants, it provides an excellent surface for the development of a keratinized, attached epithelium that withstands masticatory forces because of the increasing number and size of the connective tissue parts within it after the reconstruction surgery. The attached epithelium resembles the normal mucosa and seals the implants against the oral environment.22,29 The mucosal covering becomes rapidly populated by dendritic cells, which are major players in the initiation of specific immune responses, and this may additionally contribute to a low periimplant infection rate.22 In both reconstructive and aesthetic surgery, the facial proportions represent the gold standard of aesthetic appearance1 (Fig. 50.9, Video 50.2). Distraction osteogenesis is an inductive surgery that combines reconstructive surgery with aesthetic surgery of the face, depending on the distraction distance. In distraction osteogenesis, the gradual advancement of a bone segment leads to the formation of new bone behind it, and distraction histogenesis is the biologic process of soft tissue adaptation to the resultant gradual stretching.32 Bone transport represents an alternative to microsurgical midface reconstruction. Similar to prefabricated composite grafts, this method provides a new lining via expansion of the attached gingival tissue, which aids in the periointegration of dental implants and resists functional loading during mastication.29 In orthognathic surgery, distraction osteogenesis is best suited for the three-dimensional rearrangement of the face to optimize the facial proportions in various indications, including complex surgical protocols such as those in cleft surgery. Moreover, the muscles adherent to the distracted bone are stimulated to create new cells at the origins and insertions of the muscles as well as within the muscle mass. In addition, the bone–muscle crosstalk, which is the interaction between the regenerating muscles and the remodeling bone, improves the musculoskeletal balance of the face, leading to a better aesthetic appearance, as shown in a 28-year-old patient who had undergone unsuccessful orthognathic treatment for 7 years (Fig. 50.10). However, it must be noted that bone transport related to distraction osteogenesis across large distances may cause injury of the skeletal muscles.33 Based on the principles described previously, bone transport can be used as an alternative to microsurgical reconstruction using prefabricated composite grafts in patients with noma (see Fig. 50.9, 7). The main advantages in this setting are the requirement of fewer and cheaper surgical instruments, the shorter operation time, and the lack of a need for admission into an intensive care unit, which makes this technique applicable in developing countries, for instance, in Africa.13,17 Fig. 50.9 Possible osteotomies and regions of distraction osteogenesis (DO), with various indications for distraction in the maxillofacial region. (1) Advancement of the entire face, mostly used in syndromic patients. (2) Midface distraction in high Le Fort II or Le Fort III osteotomy. (3 and 5) Distraction of an alveolar bone block to increase the height of the alveolus. (4) Lengthening of the mandible in the sagittal dimension. (6) Distraction of the ascending branch of the mandible. (7) Bone transport. The schema should further illustrate the facial soft tissue envelope being supported by the underlying bone structure of the face. This functional musculoskeletal interaction, the “bone–muscle crosstalk,” in the face is best described as sectorial architectonic shoring (see Fig. 50.11). Fig. 50.10 Managing unfavorable results. This 28-year-old patient was treated with a comprehensive orthognathic surgical protocol including distraction osteogenesis after failure of orthodontic treatment for 7 years. (a) Disrupted facial proportions, tension on the facial soft tissue envelope with pronounced nasolabial and mentolabial folds, and “chubby cheeks” caused by displaced retaining ligaments and a loss of the alveolar bone in the piriform region and lateral maxillary segments. (b) Aesthetic appearance after skeletal rearrangement with bimaxillary orthognathic surgery including distraction osteogenesis, maxillary reconstruction by stack plasty, and restoration of musculoskeletal balance. (Reproduced from Vinzenz K, Schaudy C. Osteoplastic surgery of the face–state of the art and future aspects. Eur Surg 2011;43(5):270–283, with permission from Springer-Verlag Wien.) Fig. 50.11 Olympic Stadium, Munich (by architect Frei Otto), as an example of sectorial architectonic shoring. (2014 M(e)ister Eiskalt—Picture used under Creative Commons License.) Distraction osteogenesis has three major advantages over conventional orthognathic surgery: 1. It is possible to move segments over a longer distance, thereby reducing the need for further bone grafts. 2. It provides stable, long-term outcomes. 3. It enables the three-dimensional rearrangement of the face in the case of facial disfigurement, especially in the transverse dimension, as is needed in cleft patients.6,13 For these reasons, distraction is useful in the complex surgical protocols of cleft surgery. Moreover, a close functional relationship between the bone and soft tissue facial envelope can be achieved using distraction osteogenesis. The superficial facial fascia is cranially elongated in the neck and has deep attachments in the temporal and periorbital regions.34 This surgical anatomy of the fascia is the key to understanding the functional changes in the aesthetic appearance of the face during distraction osteogenesis. In the fat compartments of the face, the deep and superficial fascial planes are separated by areolar tissue that is adherent to both planes through a series of dense fibrous attachments.35 The fascia with its viscoelastic properties is normally considered a passive structure that transmits mechanical tension generated by muscular activities.36 Advanced bone relocation surgery changes the tension on the fascia and the superficial musculoaponeurotic system (SMAS) via retaining ligaments, which function as sectorial architectonic shoring over the fat compartments (Fig. 50.11). As a consequence, this leads to greater primary tension on the SMAS and fixed mimic muscles.
50
Complex Soft Tissue and Bony Maxillofacial Reconstruction
Avoiding and Managing Unfavorable Results in Complex Soft Tissue and Bony Maxillofacial Reconstruction
Evolution of Reconstructive Maxillofacial Surgery to Avoid Unfavorable Results


Reconstruction with Prefabricated Grafts
Prefabricated Composite Mandibular Grafts in Orofacial Reconstruction
Surgery for Midface Defects
Regenerative, Inductive Maxillofacial Surgery
Induction of Tissues in Prefabricated Grafts
Induction of an “Osseomucosal Unit”
Complete Restitution of the Inner Mucosal Lining
Attachment of the Gingiva to Resist Masticatory Load
Anti-inflammatory Immune Response of the Neomucosa
Distraction Osteogenesis and Histogenesis
Bone Transport

Distraction Osteogenesis in Orthognathic Surgery
Musculoskeletal Balance in Distraction Osteogenesis
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine