A woman presents after Mohs excision of a basal cell carcinoma within the right alar. A composite defect of her right upper lip, cheek, and ala is present. Although distressed, her concerns are somewhat alleviated by the prior successful reconstruction of a full-thickness defect of her left ala, some years previously. This content presents the principles of the repair, the surgical plan, and details of the multiple procedures performed for successful reconstruction.
Analysis of the defect and decision making
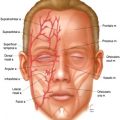
On physical examination ( Fig. 1 ), a faint vertical left paramedian forehead scar, which followed the previous reconstruction, is visible. The forehead is otherwise high and expansive.

The left ala appears normal, although it is not. Some years previously, the patient presented with a full-thickness defect of the left entire ala and part of the inferior sidewall. Adjacent lip and cheek were uninjured. The defect had been repaired with a 3-stage folded forehead flap for cover and lining, with a delayed, primary, ear cartilage alar margin buttress graft to support, shape, and brace the left nostril margin. Following subunit principles of nasal reconstruction, the normal intact right ala had been used as a guide to design a template with the correct dimension and outline of the contralateral normal ala. The right ala was used to plan the exact replacement of the entire left ala and a few millimeters of the left tip subunit with a vertical forehead flap. A distal extension, about 1.5 cm wide and 7 mm long, was added to the distal covering flap. The extension was folded inward to replace the missing lining. During an intermediate operation 1 month later, the covering flap was elevated completely off the nose with 2 to 3 mm of subcutaneous fat. The distal folded lining was now healed to the adjacent residual nasal lining and was no longer dependent on the supratrochlear pedicle for blood supply. The underlying doubly layered excess of subcutaneous fat and frontalis areolar tissue was excised, exposing thin supple vascular lining. The contralateral normal alar template was then used to design a precise alar margin graft to shape the left nostril margin. The graft was fixed to the restored lining. The thin forehead flap was then returned to the recipient site. One month later, the pedicle of the flap was divided. During a subsequent revision, the left alar crease was further refined through a direct incision to sculpt a flat sidewall, a deep alar crease, and a convex alar contour. The slightly thick rim margin was thinned by excising excess soft tissue between the lining and cartilage graft through the old incision present along the nostril margin.
A short transverse scar is visible within the superior dorsum at the site of a previous skin cancer excision that was closed primarily.
The new defect involves several facial units but is more superficial.
Anatomically, the skin is missing over the entire ala, part of the inferior sidewall, and the adjacent medial cheek and lateral lip. Soft tissue within the cheek over the piriform aperture has been excised. The normal fibrofatty middle layer support of the ala is gone. Nasal lining is intact.
Aesthetically, the complex midface has been destroyed. The expected color and texture, landmark outline, and 3-dimensional shape are abnormal. Because the underlying orbicularis muscle is present, if skin is restored to cover the lip, the lip will function normally.
The face can be divided into geographic areas of characteristic skin quality, border outline, and 3-dimensional contour. The cheek is a peripheral unit, largely flat and expansive with a variable border outline that is not completely seen on frontal view. The nose and upper lip are central units and are exactly contoured and outlined. An abnormality in a part of the lip or cheek is quickly apparent because the contralateral remaining lip or cheek creates a visually disturbing comparison.
The nose sits on a facial platform of the cheek and lip. The nasolabial fold separates the round fullness of the medial cheek and the flat upper lip. The nasolabial fold does not extend into the alar crease but is separated from the crease by a hairless triangle of skin, which lies adjacent to the alar base inset. The nose sits on the facial platform in an exact position and projects with specific angles.
The nose is divided into subunits. The flat sidewall is separated from the round convex ala by the alar crease. The alar subunit is outlined by the nostril margin inferiorly, the alar crease superiorly, the slight alteration in contour with the soft triangle and tip subunits medially, and the alar groove laterally where the ala is inset into the lip at the alar base.
Each facial unit must be restored in terms of its own quality, outline, and contour and in relationship to the other facial units. The dimension, volume, position, projection, platform, skin quality, border outline, and 3-dimensional contour of the midface must be reestablished.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


