Key Words
tendon transfers, median nerve palsy, radial nerve palsy, ulnar nerve palsy, claw hand
Synopsis
Tendon transfers can be used to restore hand and wrist function after a nerve injury, both in the acute setting and in delayed presentations. Injuries of the brachial plexus and peripheral motor nerves are common indications for tendon transfers. Alternatively, patients may have loss of a muscle-tendon unit (MTU) from trauma or after an oncologic resection; reconstruction with a tendon transfer can replace the function of the lost MTU. Tendon transfers can also restore function after attritional tendon ruptures, which are most commonly seen in rheumatoid arthritis.
Clinical Issues
Tendon transfers are used to restore the function of a paralyzed or lacerated MTU using a nearby functional MTU. They can be used in the upper and lower extremity. In the upper extremity, they are most commonly used to restore flexion and extension of the wrist and fingers and less frequently used for the shoulder and elbow.
Tendon transfers in the upper extremity can restore function after the loss of an MTU function caused by injury of the central or peripheral nervous system, closed rupture or open injury to the MTU, and various diseases. Infectious diseases, such as poliomyelitis, can cause damage to motor neuron ganglia and subsequent muscle paralysis. Inflammatory arthropathies, most commonly rheumatoid arthritis, can be complicated by attritional tendon ruptures. Some patients with hand spasticity, for example due to cerebral palsy, can benefit from carefully selected tendon transfers.
Patient presentation varies based on the etiology of the MTU loss. Mixed peripheral nerve injuries present with sensory and motor losses in the affected nerve distribution. Patients with traumatic MTU deficits have a history of injury to the affected MTU. Lacerations or fractures can result in discontinuity of an MTU. Primary MTU repair is preferred; however, if not possible or if unsuccessful, tendon transfers can be used for reconstruction. Nerve lacerations can be repaired acutely or can be reconstructed with nerve transfers up to approximately 12 months after injury; better outcomes are seen with earlier nerve surgery. In the case of a delayed nerve injury presentation or failed nerve repair, tendon transfers are options to restore function.
In rheumatoid arthritis, the ulnar dorsal tendons (extensor digiti minimum [EDM], extensor digitorum communis [EDC]) are most commonly ruptured, due to attrition over a dorsally prominent ulnar head. The flexor pollicis longus (FPL) can rupture due to chronic attrition over a volar osteophyte on the scaphoid known as a Mannerfelt lesion. Rheumatoid arthritis patients typically have systemic disease symptoms, and multiple joints are involved.
Traumatic nerve and MTU injuries affect the balance between the flexor and extensor muscle groups of the upper extremity. This can lead to asynchronous and weak function. Tendon grafts, tendon transfers, nerve transfers, and free muscle transfers can be used for upper-extremity reconstruction. The risks and benefits of each technique must be considered and each patient treated with an individualized plan.
Tendon transfers are reliable, with minimal donor site morbidity. They restore function early after surgery; range of motion (ROM) exercises are started 4 weeks post-operatively, and unrestricted activities are permitted 12 weeks post-operatively. In contrast, nerve transfers often require 6 to 9 months before clinical evidence of muscle reinnervation is seen and up to 2 to 3 years for maximal recovery. Local MTUs are transferred in tendon transfers, negating the need for microsurgery expertise and equipment that are needed for free muscle transfers. Tendon grafts can be used when there is a tendon gap in the MTU. However, when the MTU lacks innervation or is severely damaged, a tendon graft is insufficient to restore function, and a tendon transfer is required.
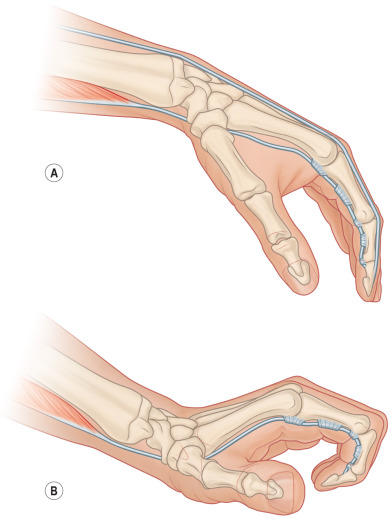
A careful physical examination documents missing functions and intact MTUs. In theory, any MTU can be transferred; however, donor site morbidity must be considered, and therefore certain MTUs are more appropriate for transfer than others ( Table 5.6.1 ). Synergistic transfers (such as the use of a wrist extensor for finger flexion) are the most intuitive for patients to learn and offer the quickest return of function ( Fig. 5.6.1 ). A redundant MTU is transferred that minimizes donor site morbidity while restoring a lost function. Finding an appropriate donor MTU is more difficult in combined nerve injuries because more muscles are affected, causing a greater number of functional deficits with fewer intact MTUs available for transfer.
| Principle of Tendon Transfer | Description |
|---|---|
| Expendable donor | When selecting an MTU for transfer, any resulting weakness must be considered. One MTU must remain intact to perform the donor’s original function. For example, if the FCR and PL are transferred, the FCU must be preserved to maintain wrist flexion. |
| Straight line of pull | A direct line of pull maximizes the power of the tendon transfer. End-to-end suturing with Pulvertaft weaves is preferred. If a direction change is unavoidable, the tendon should be passed around a fixed structure that behaves as a pulley. |
| One muscle for one function | To maximize the power of the tendon transfer, each transferred tendon should be used to restore one function only. One MTU can restore the same function in multiple digits. For example, finger extension can be restored by transferring one donor MTU, such as the FCR, to the four EDC tendons. |
| Similar force of contraction | A donor MTU of similar strength as the recipient MTU (before injury) will permit restoration of function without affecting the balance and resting posture of the limb. On transfer, the donor MTU loses one Medical Research Council (MRC) grade of strength; MRC5 muscles are preferred as donors. |
| Adequate excursion | The donor MTU should have a similar excursion as the tendon that it is replacing. Finger flexor tendons (FPL, FDP, FDS) have 7 cm of excursion. Finger extensor tendons (EPL, EIP, EDC, EDM) have 5 cm of excursion. Wrist flexors (FCR, PL, FCU) and extensors (ECRL, ECRB, ECU) and the BR have 3.3 cm of excursion. The tenodesis effect increases excursion for tendon transfers crossing the wrist ( Fig. 5.6.1 ). |
| Synergism | Synergistic transfers are preferred. Synergistic muscle groups normally function together; this facilitates rehabilitation. Wrist flexion is linked with finger extension. Similarly, wrist extensors are synergistic with finger flexors. |
| Balance more important than strength | Balance between hand and wrist flexion and extension is critical. For example, imbalances between strong wrist flexors and weak wrist extensors lead to poor wrist extension. This impairs finger flexion, which limits hand grasp and overall hand function. |
| Stable, supple soft tissue bed | To permit tendon gliding, a transferred tendon should pass through tissue that is neither inflamed, edematous, nor scarred. |
| Skeletal stability | A stable platform with adequate bone and joint stability is required before tendon transfer. If required for patients with combined nerve lesions, arthrodesis of select joints is performed before tendon transfer. |
| Full passive range of motion | All joints must be supple before tendon transfer reconstruction to optimize outcomes; a tendon transfer will not restore ROM if the joint is stiff. Intensive hand therapy is often required to maximize passive ROM before surgery. If necessary, joint contracture release is performed before tendon transfer. |
Management
A comprehensive history and physical examination will identity the patient’s functional deficits and their reconstructive goals. Selection of an appropriate donor MTU for transfer is important to restore function while minimizing donor site morbidity. The patient’s handedness, occupation, and avocations are discussed. Any limitations in the patient’s activities of daily living, recreation, and work are documented.
To determine the level of injury of the MTU, the skin is examined; any previous lacerations are noted. Acute tendon lacerations are typically repaired with direct tendon repair, but these injuries can be missed. Palpating for the point of maximal tenderness along the tendon can indicate the level of tendon injury and subsequent tendon retraction; this finding is most pronounced early after a tendon injury and can be absent in late presentations. For closed tendon ruptures, ultrasound can be helpful to determine the location of the injury. After a nerve injury, the MTU is in continuity, but lacks innervation.
To maximize the strength of the tendon transfer and to allow early active ROM, tendon transfers are best secured using 3 Pulvertaft weaves. The donor tendon is divided distally and the recipient tendon is divided proximally to facilitate adequate tendon weaving. Setting the tension of the tendon transfer is critical for restoration of function while preventing the loss of ROM of other joints. The tension is set with 1 Pulvertaft weave, and then the tenodesis effect is checked to ensure adequate ROM. Adjustments in tension can be made with the second and third Pulvertaft weaves. Each Pulvertaft weave is secured with a minimum of two non-absorbable sutures; we prefer to use 3-0 polyester suture.
Tendon transfers can be performed in an end-to-end or end-to-side fashion. End-to-end suturing facilitates a direct line of pull and is used if the recipient tendon is not expected to have any spontaneous recovery; for example, after complete denervation from an unrepaired nerve transection. If the nerve has been repaired and some muscle recovery is expected, the tendon transfer is performed in an end-to-side fashion to augment existing function.
Techniques
Trauma Reconstruction
Thumb Extension
The extensor pollicis longus (EPL) can be sharply lacerated in an open injury or can be ruptured in a closed injury. There is a 5% incidence of EPL tendon rupture after a non-displaced distal radius fracture. In these cases, edema and bleeding raise the pressure in the tendon sheath, compromising the tendon’s vascular supply, which can lead to avascular necrosis of the tendon and its subsequent rupture.
The extensor indicis proprius (EIP) is the most commonly transferred tendon to the EPL to restore thumb extension. Other donors include the palmaris longus (PL) and the flexor digitorum superficialis (FDS) from the middle or ring finger.
If selected as a donor, the EIP tendon is harvested through a transverse or a V-shaped incision over the dorsal index finger metacarpophalangeal joint (MCPJ). To prevent an extension lag of the index finger, the remaining distal stump of the EIP can be sutured end-to-side to the EDC of the index finger over the MCPJ.
The EIP is retrieved through a 2-cm longitudinal incision distal to the extensor retinaculum over the dorsal wrist. An additional longitudinal incision is made over the distal third of the thumb metacarpal. The EIP tendon is routed subcutaneously to this incision. With the wrist in neutral and the thumb fully extended, the EIP is transferred to the EPL tendon and secured using Pulvertaft weaves.
Thumb Flexion
Laceration or rupture of the FPL tendon results in the loss of thumb interphalangeal joint (IPJ) flexion and key pinch. This function can be restored by the transfer of the brachioradialis (BR) or FDS of the middle or ring fingers.
Brachioradialis transfer.
In the BR transfer, an incision is made over the volar-radial distal radius to identify the FPL as well as the insertion of the BR onto the radial styloid. The BR tendon is harvested distally with a periosteal extension from the distal radius to increase its length. The superficial branch of the radial nerve is protected. The BR is dissected and freed proximally to maximize its excursion. It is moved volarly and secured to the FPL proximal to the carpal tunnel. The tendon transfer tension is set with the elbow flexed at 90 degrees, the wrist in 20 degrees of extension, the forearm fully pronated, and with the thumb pulp and proximal interphalangeal joint (PIPJ) of the index finger touching.
Flexor digitorum superficialis transfer.
Alternatively, the middle or ring finger FDS can be harvested and retrieved through transverse incisions at the base of the proximal phalanx and the proximal palm. It is then tunneled to the FPL with the aid of a fine catheter. If the distal FPL is absent and the FPL tissue bed is scarred, a two-stage tendon reconstruction should be performed with the FDS; the FDS is longer than the BR and can reach the distal phalanx of the thumb. In the first surgery, a silicone rod is placed to create a new sheath for the FPL. In the second stage, the FDS tendon is passed into the newly formed sheath and secured to the base of the distal phalanx of the thumb using a suture anchor or a button-fixed, pullout suture.
Finger Extension
Common tendons used to restore finger extension include the flexor carpi radialis (FCR) and the ring finger FDS. Either of these tendons can be transferred to the EDC to restore extension of the index, middle, ring, and small fingers. All fingers can be reconstructed or only the affected fingers in incomplete EDC injuries.
The middle and ring finger FDS tendons have greater excursion (7 cm) than the FCR (3.3 cm), enabling full excursion of the EDC tendons (5 cm). Potential disadvantages of an FDS harvest are a weakened grip and a swan-neck deformity of the donor finger(s) because of a lack of restraint by the FDS at the PIPJ. The risk of a swan-neck deformity can be minimized by performing an FDS tenodesis to the neck of the proximal phalanx after distal FDS division.
Flexor carpi radialis transfer.
Two incisions are used. The first is made over the volar radial distal forearm to harvest the FCR tendon distally at its insertion on the volar base of the second metacarpal. A second incision is made over the dorsal distal forearm to expose the fourth extensor tendon compartment containing the EDC and EIP tendons. The FCR tendon is passed subcutaneously from the volar to the dorsal wrist, around the radial wrist, and under the skin bridge between the two incisions for transfer to the EDC proximal to the extensor retinaculum. The subcutaneous tunnel must be dissected proximally and made sufficiently large to create a direct line of pull of the FCR tendon. Tension is set for this transfer with the FCR tendon under maximum tension, the wrist held in neutral, and the MCPJs fully extended.
Flexor digitorum superficialis transfer.
A transverse incision is made over the volar base of the ring finger to expose the FDS tendon for division distal to the A2 pulley and proximal to Camper chiasm.
The FDS tendon is routed subcutaneously around the ulnar wrist to the EDC tendons for transfer. A longitudinal incision, just ulnar to Lister’s tubercle over the dorsal wrist and proximal to the extensor retinaculum, is used to expose the EDC tendons. The transferred FDS is sutured to the EDC tendons with the FDS under maximum tension with the wrist in 20 degrees of extension and the hand held in a fist.
Finger Flexion
The function of the flexor digitorum profundus (FDP) tendons can be restored by transferring the extensor carpi radialis longus (ECRL). A tendon graft may be required to lengthen the ECRL. An incision is made over the dorsal base of the index finger metacarpal to expose the ECRL insertion. The tendon is harvested at this site and then mobilized proximally to a second incision over the dorsal radial forearm. It is then re-routed subcutaneously around the radial border of the forearm and sutured into the affected FDP tendons proximal to the carpal tunnel using a third incision. Tension is set to restore the flexion cascade of the digits; the tension is set progressively tighter as one moves from the index to the small finger.
Alternatively, if one to two FDP tendons are nonfunctional, they can be transferred end-to-side to the adjacent functional FDP tendons.
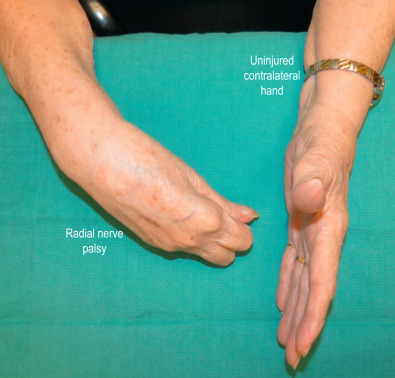
Radial Nerve Palsy
An injury proximal to the elbow, to the radial nerve proper is termed a high radial nerve palsy. Extension of the wrist, fingers, and thumb is lost ( Fig. 5.6.2 ). Abduction of the thumb is also impaired. The inability to extend the wrist leads to a weakened grip. The inability to extend the fingers and thumb makes it difficult for patients to grasp objects. Tendon transfers aim to restore wrist, finger, and thumb extension.