Common Clinical Presentations
 INTRODUCTION
INTRODUCTION
There are many illustrative cases in each of the chapters on treatment, but several clinical situations are common enough to warrant special presentation. In addition, there are some more unusual presentations that are commonly misdiagnosed. These are important for the clinician to recognize and are presented here.
CASE NO. I—AXIAL VARICOSITIES IN A YOUNG MALE
A 29-year-old computer networking consultant who travels extensively presents with varicose veins present since the age of 20 years and painful for the last two years. He noticed the initial onset while playing tennis. Both parents have a history of varicose veins. The presenting veins are situated along the anterior surface of the left thigh and the medial surface of the left lower limb.
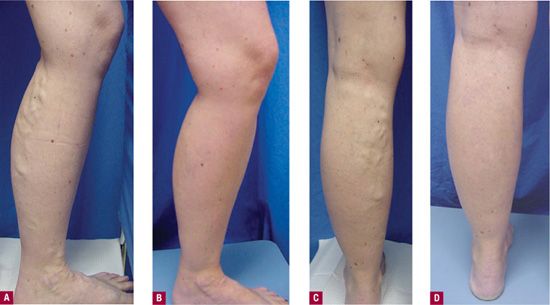
EXAM On the left leg, a varicose vein is visible and palpable extending from the upper anterior thigh (not to the groin) down to the knee. Another large varicose vein is seen originating at the medial calf length (mean diameter: 12 mm). Percussion allows a fluid wave to be felt on the thigh portion when the calf portion is tapped repeatedly (Figures 7-1A and 7-1B).

![]() FIGURE 7-1 A. Thigh varicosities before treatment. B. Calf varicosities before treatment. C. Recurrence of calf varicosities (although smaller) two years after initial sclerotherapy.
FIGURE 7-1 A. Thigh varicosities before treatment. B. Calf varicosities before treatment. C. Recurrence of calf varicosities (although smaller) two years after initial sclerotherapy.
DOPPLER No incompetence is noted at the left saphenofemoral junction (SFJ), even with Valsalva maneuer. Marked incompetence is heard along the entire visible vein, in the region of the great saphenous vein (GSV) at the level of the knee, and in the lower segment of the varicosity in the calf. There is no reflux in the left small saphenous vein (SSV).
FUNCTIONAL TESTS Digital-Photoplethsmography (D-PPG) shows refill time of 19 s.
DUPLEX A Duplex ultrasound examination is ordered with a registered vascular technician knowledgeable in the superficial venous system, but the patient’s insurance plan only pays for a Duplex examination at a specific radiology group. The examination report reads, “No evidence of deep venous thrombosis. Reflux seen in some superficial veins.”
TREATMENT On the basis of the fact that the patient does not desire surgery nor is reflux detected at the SFJ by the general radiologist’s Duplex technician, the patient is treated with 3 percent STS (sodium tetradecyl sulfate) injections of 1 cc at three sites total. At one month, significant reduction of the diameter of the varicosities is noted. A second treatment is performed with 1 percent STS at six sites. A follow-up one month later shows complete resolution.
LONG-TERM FOLLOW-UP The patient returns in 2 years with a slight recurrence in the calf (Figure 7-1C). Duplex examination reveals reflux at the SFJ and along the GSV. Treatment consists of ligation at the SFJ followed by stripping of the thigh portion of the GSV. The calf varicosity is injected 1 month after surgery with 1 percent STS. The patient remains free of disease at five years.
COMMENTARY Reflux in the anterolateral tributary of the GSV extended down the leg to cause reflux in a branch varicosity of the calf. Recurrence at 2 years was due to either new development of reflux in the GSV related to genetic susceptibility or to the possible failure to diagnose SFJ incompetence initially because of an inadequate Duplex examination.
CASE NO. II—AXIAL VARICOSITIES IN A MIDDLE-AGED WOMAN
A 40-year-old woman complains of leg pain and swelling of both legs that has become progressively worse during and after four pregnancies. In addition, she complains that her both legs have veins that bulge and ache constantly. She also has symptoms of leg heaviness, fatigue, and a sensitivity to touch. Family history is positive for a mother and sister with varicose veins. Past medical history is negative.
EXAMINATION Prominent varicosities from her left medial knee extending down to the ankle and foot are observed (Figure 7-2A). A posterior view of the left varicosity extending over the posterior calf is observed in Figure 7-2C. A small varicosity was visible on the right medial calf.
![]() FIGURE 7-2 A. Left medial varicosities before treatment. B. Improvement of left leg varicosities. C. Left posterior calf varicosities before treatment. D. Improvement of left posterior calf varicosities.
FIGURE 7-2 A. Left medial varicosities before treatment. B. Improvement of left leg varicosities. C. Left posterior calf varicosities before treatment. D. Improvement of left posterior calf varicosities.
DUPLEX ULTRASOUND The right GSV is incompetent from zone 3.0 to zone 5.5 where an incompetent medial branch arises. The right SSV is normal. The left GSV is competent throughout its entire course. The left SSV is incompetent from zone 5.0 to zone 6.5.
ASSESSMENT This patient has venous insufficiency that requires endovenous treatment. The patient had her right GSV and her left SSV treated with 1320 nm endovenous laser ablation. She also had one session of duplex-guided foam sclerotherapy in each leg at 6 weeks status after successful ablation of the veins. Significant improvement is noted after the procedure (Figures 7-2B and 7-2D).
COMMENTARY It is important to screen both legs with ultrasound when patients have prominent symptoms and a strong family history. Her physical examination only noted a small area of bulging veins on the right leg, yet she had an incompetent GSV causing her leg symptoms. A close follow-up is important in young patients with history of venous insufficiency to check for new areas of insufficiency.
CASE NO. III—NEW ONSET OF A PAINFUL VEIN IN A TEENAGER
A 17-year-old female develops a varicose vein during puberty. Family history is noncontributory. The patient presents for treatment due to the appearance of varicose vein, as there are no symptoms.
EXAMINATION Inspection reveals a blue varicose vein on the medial calf in Boyd’s region (Figure 7-3A). Palpation and percussion do not reveal a varicose GSV or SSV.
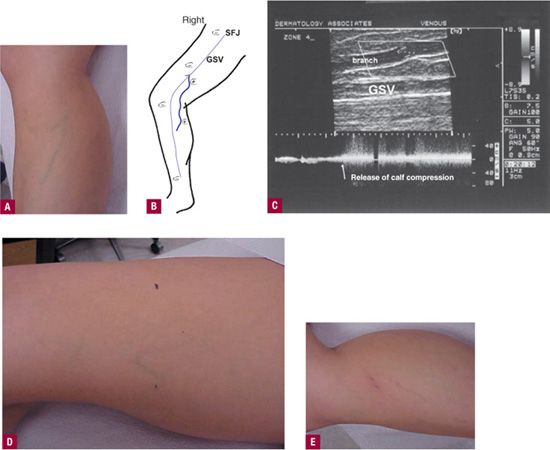
![]() FIGURE 7-3 A. Varicosity before treatment. B. Mapping of Duplex findings. C. Duplex image of the incompetent branch off of the GSV. D. Markings on thigh prior to Duplex-guided sclerotherapy. E. Vein contraction and erythema immediately after injection.
FIGURE 7-3 A. Varicosity before treatment. B. Mapping of Duplex findings. C. Duplex image of the incompetent branch off of the GSV. D. Markings on thigh prior to Duplex-guided sclerotherapy. E. Vein contraction and erythema immediately after injection.
DOPPLER Doppler auscultation demonstrates reflux in the visible varicose vein, with some reflux detectable in the thigh. Both saphenous veins are competent at the junctions and below.
FUNCTIONAL TESTS These are not performed in this case.
DUPLEX EXAMINATION Due to the reflux detectable in the thigh on Doppler examination, a Duplex examination is performed showing a medial branch varicosity originating off the GSV in the thigh extending directly to the visible varicose vein. Figure 7-3B shows the mapping of Duplex findings; the Duplex image of the incompetent branch off of the GSV is seen in Figure 7-3C.
TREATMENT Duplex-guided sclerotherapy in the thigh is performed; 1 percent STS is used at origin of the branch point (Figure 7-3D), followed by 0.2 percent STS injection in the visible portion of the vein. Visible disappearance and contraction are noted immediately (Figure 7-3E). Complete resolution occurred after one treatment.
COMMENTARY Even a patient as young as 17 years can develop a single branch varicosity in the thigh leading to a “reticular” varicose vein on the medial aspect of the calf. In this early stage, it could be efficiently and effectively treated by Duplex-guided sclerotherapy with just one treatment.
CASE NO. IV—LATERAL VENOUS SYSTEM
A 46-year-old woman complains of the appearance of the veins on her lateral thigh. These had developed during pregnancy, and gradually worsened over the preceding 15 years. No significant symptoms were noted.
EXAMINATION Clinical examination reveals a prominent blue reticular vein network with associated telangiectasias of the lateral thigh that faded from sight below the knee. No other abnormal veins were observed (Figure 7-4A).

![]() FIGURE 7-4 A. Lateral venous system before sclerotherapy. B. Lateral venous system after sclerotherapy.
FIGURE 7-4 A. Lateral venous system before sclerotherapy. B. Lateral venous system after sclerotherapy.
DOPPLER Doppler auscultation reveals mild reflux along the lower course of the reticular vein, loudest near the lateral knee.
FUNCTIONAL TESTS These tests are not performed in this case.
DUPLEX ULTRASOUND Duplex is not performed in this case.
ASSESSMENT Incompetent lateral venous system manifesting in prominent reticular veins and some associated telangiectasias.
TREATMENT Prior to evolution of foam sclerotherapy, a series of two treatments are performed. The first uses 1 percent STS, 0.3–0.5 cc, into each of several sites 4–6 cm apart along the reticular veins with a total of 4 cc, and the second uses 0.1 percent STS, 0.5 cc, into each group of telangiectasias with a total of 3 cc. Compression hosiery (18–20 mmHg at the ankle) are worn for two weeks after each treatment.
At the second treatment, the reticular veins have greatly shrunk. A few hyperpigmented nodular areas are drained of blood (see Chapter 24). A total of 3 cc of 0.5 percent STS are injected into the remaining reticulars, and a total of 1.5 cc of 0.1 percent STS into the telangiectasias. After two months, the leg has cleared nicely (Figure 7-4B).
COMMENTARY This patient is an example of the commonly seen pattern of an abnormal lateral venous system without other venous abnormalities that usually responds extremely well to compression sclerotherapy. Present-day therapy would halve the concentrations in favor of foamed sclerosant.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


