Commissure Reconstruction: Overview
H. G. THOMSON
EDITORIAL COMMENT
Because this chapter provides a comprehensive review of the various techniques described for commissure reconstruction, the names of authors have been included. In most other chapters, we have tried to avoid lengthy lists of historical details. These have instead been referred to the list of references.
Bakamjian (1) in 1964 stated that molding the lip commissure with functional fidelity is an almost impossible task. The aim of surgical reconstruction is to give symmetry to the commissure in repose and to permit full opening without webbing. The former goal is much easier to attain than the latter. The subtle flow line of the red lip to its termination at the angle of the commissure and its ability to move up, down, and laterally, as well as vertical mucosal stretching, were well described by Stricker in 1981 (2). The Z distribution of the skin and the accordion effect of the mucosa were emphasized. To achieve this is the goal of reconstructive surgery, but the most common shortfall is the apparent fullness in the commissure owing to a lack of contouring.
INDICATIONS
Defects of the commissure apex are rare; most problems are pericommissural in nature and involve the apex. The most common indication is trauma, especially electrical oral burns.
ANATOMY
To apply the tenets of reconstruction properly, we must first appreciate the topographic location of the commissure on the face. Broadbent and Matthews (3) described the normal location of the oral commissure. With the normal in mind, various landmarks can be chosen and methods for locating the apex of the proposed commissure can be applied (Fig. 180.1). There should be a special awareness of the tapering effect of the commissure, and this begins at a vertical line through the medial canthus.
FLAP DESIGN AND DIMENSIONS
Tongue Flaps
Bakamjian (1) described several types of tongue flap designs, in particular a ventrolateral, anterior-based flap, which he included in commissure reconstruction as part of partial or total red lip reconstruction after cancer ablation. Guerrerosantos et al. (4) in 1963 were really the first authors to describe the use of a tongue flap that could give not only mucosal functional and aesthetic advantages but also a degree of much needed bulk in the area. They also described the microscopic papillary appearance of
tongue mucosa, which, after 20 to 90 days, takes on a smooth red lip appearance. They usually used the tongue tip.
tongue mucosa, which, after 20 to 90 days, takes on a smooth red lip appearance. They usually used the tongue tip.
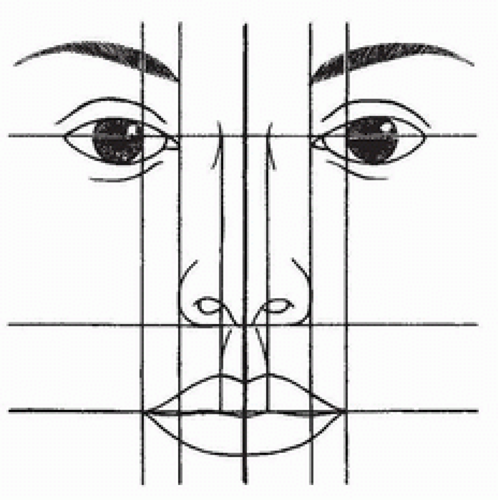 FIGURE 180.1 Wright’s facial landmarks for commissure location. |
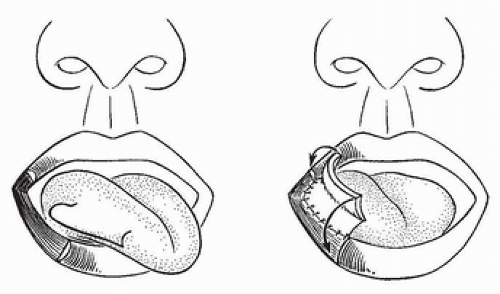 FIGURE 180.2 Converse type of tongue flap for commissure reconstruction. |
McGregor (5) also described a tongue flap. Jackson (6) reported the use of tongue flaps in oral electrical burns and the need for awareness of the fact that the tongue flap can be separated by young patients’ sharp teeth. To prevent this, he fabricated a prophylactic bite block. He reported an anterior-based sublingual flap that required lanolin three times a day for a few months to prevent desiccation. Jackson makes a point that the tongue papillae do not always disappear, and therefore, his sublabial flap, which is smooth and less red, provides better cosmetic coverage.
In 1974 Zarem and Greer (7) described a sublabial or ventral flap that is anteriorly based and applied to only one surface of the commissure; the other surface is closed with simple mucosal advancement. They did this in an attempt to reduce ultimate bulk excess. They emphasized the shortfall of the color match provided by the vivid pink of the tongue mucosa. They prefer this reconstruction to be initiated 3 weeks after injury and have found that the pedicle can be separated at 2 weeks. A similar technique was reported by Converse in 1977 (8) (Fig. 180.2). In 1980 Ortiz-Monasterio and Factor (9) described an anterior-based, split, lateral sublabial tongue flap for commissure reconstruction that provides significant tissue to the commissure area and, indeed, may create difficult problems with debulking (Fig. 180.3).
Cheek Flaps
Reconstructions of the lips with cheek flaps are legend. Those related to the commissure only are somewhat limited in number and relate to primary tumor resection and reconstruction. Tumors of the commissure constitute fewer than 6% of those involving the lip area. Zisser (10) in 1975 reported a technique for cheek advancement and mucosal flap reconstruction of the commissure. The deepithelialized flaps are rotated up into the defect to give both bulk and alignment (Fig. 180.4). Brusati (11) in 1976 described a similar technique for commissure reconstruction (Fig. 180.5) that is also based on a Burow’s triangle principle. Attempts are made to keep the major scar lines in the axis of the smile crease. This flap is more suitable for horizontal defects compared with the Zisser flap, which is more applicable to vertical problems.
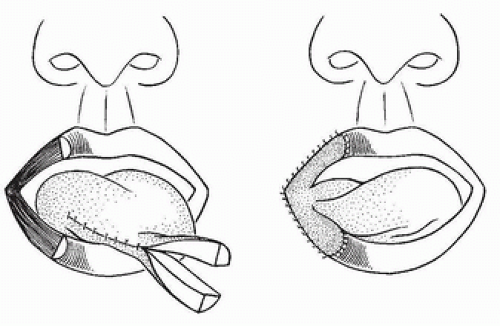 FIGURE 180.3 Ortiz-Monasterio and Factor split pedicle tongue flap. |
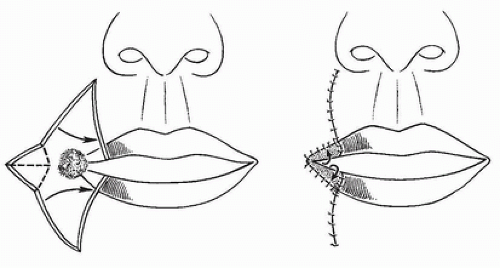 FIGURE 180.4 Zisser method of advancement commissure reconstruction for vertical defects.
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Inferior Turbinate Flap for Closure of Septal Perforations Inferior Turbinate Flap for Closure of Septal Perforations
 Galeal Flaps Galeal Flaps
 Paired Deltopectoral Skin Flap to The Lip Paired Deltopectoral Skin Flap to The Lip
 Microvascular Free Transfer of Serratus Anterior and Rib Composite Flap Microvascular Free Transfer of Serratus Anterior and Rib Composite Flap
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|