Commissure Reconstruction
R. V. ARGAMASO
EDITORIAL COMMENT
The technique demonstrated here is a functional restoration of the commissure, which should be kept in mind for relatively large defects, particularly following cancer resection. On the other hand, for children who occasionally suffer from electrical burns of the commissure, the simple technique of an angle prosthesis to stretch the area and to soften the scar tissue should also be considered.
The lips form an aesthetic unit of the face and are multifunctional. When an electrical burn occurs at the commissure of the mouth (an injury more likely to be acquired by inquisitive infants and young children), some functional impairment and structural asymmetry may result. Deep burns disrupting the orbicularis oris muscle are a challenge to adequate reconstruction (1).
INDICATIONS
The vermilion tapers and disappears at the corners of the mouth. A full-thickness destruction of tissue at the commissure invariably includes muscle fibers. As a consequence, the normally closed interval between the lips at the corner when the mouth is at rest is transformed into a gap. During the acute
stage of the injury, this corner of the mouth becomes incompetent and allows continuous drooling of saliva, which is both untidy and unsightly.
stage of the injury, this corner of the mouth becomes incompetent and allows continuous drooling of saliva, which is both untidy and unsightly.
An acute injury is treated conservatively to allow healing with the least sacrifice of viable tissue. As a result of scar deposition and contracture, the oral circumference is reduced. The resulting postburn microstomia is disfiguring and, in severe cases, causes feeding difficulties.
ANATOMY
The orbicularis oris muscle, unlike the orbicularis oculi, is formed by complex strata of muscle fibers surrounding the mouth. These fibers originate from other muscles of the face and therefore come from several directions.
At the commissure, the buccinator sends upper and lower fibers to the upper and lower lips, respectively. Its middle fibers decussate with those of the levator anguli oris to pass to the lower lip and with those of the depressor anguli oris to pass to the upper lip. The zygomaticus inserts obliquely into the angle of the mouth and blends with the levator and depressor anguli oris. The risorius runs horizontally and inserts into the constituted orbicularis muscle and the skin at the corner of the mouth. These muscles are innervated by the buccal branches of the seventh nerve.
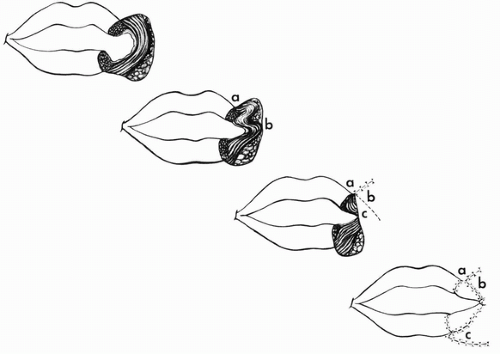 FIGURE 181.1 Stages in reconstruction of the commissure (see text).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





