Composite breast augmentation is a simple procedure combining the ability of an implant to provide increased volume with the reshaping possibilities offered by fat grafting. The ability to camouflage the implant allows use of a premuscular, retrofascial pocket, avoiding the disadvantages and morbidity associated with retromuscular positioning.
Key points
- •
Composite breast augmentation (CBA) offers an attractive alternative to the use of submuscular implants in patients of slender stature.
- •
CBA has the advantage of providing increased breast volume, while simultaneously maintaining a natural appearance.
- •
By avoiding submuscular implant positioning, postoperative pain is reduced, as is dynamic movement of the implant.
Introduction or overview
For over 10 years, numerous investigators have described the successful and extensive use of fat grafting in plastic surgery. The original concept of fat micrografting can be attributed to Coleman. Through his work, liposculpture and its benefits were introduced, initially in the face, followed by grafting to the breast and body. The evolution of micrografting was further supported by the work of Yoshimura and colleagues in their sentinel article discussing cell-assisted lipotransfer for cosmetic breast augmentation. Throughout the history of fat grafting, concerns have been raised regarding its safety in postoperative surveillance of breast architecture. Such concerns have been addressed by Delay and colleagues who demonstrated that fat grafting does not in fact interfere with mammographic interpretation. Rubin and colleagues demonstrated that fat grafting of the breast produced fewer radiographic abnormalities and improved Breast Imaging Reporting and Data System (BI-RADS) scores with less-aggressive follow-up recommendations by breast radiologists when compared with reduction mammoplasty, a widely accepted procedure. Cameron and colleagues had comparable conclusions with their series of patients operated with the CBA technique. The significant contributions of Khouri and colleagues must also be recognized. In this article by Khouri and colleagues, they introduce the BRAVA device (Brava, LLC, a subsidiary of Bio-mecanica Inc, Miami, FL, USA), which, when used in combination with fat grafting, improves fat engraftment by enlarging the capacity of the recipient site and enhancing the vascularity of the breast.
Although this list is by no means exhaustive, it certainly demonstrates the pivotal role fat grafting has in modern plastic surgery and recognizes the numerous surgeons who have contributed to its evolution. Interest in fat transfer is not new, as well summarized by Mazzola elsewhere in this issue. However, it can be said that the first technical refinements made by Coleman, followed by many other contributors, have not only significantly improved the quality of results but also broadened the indications.
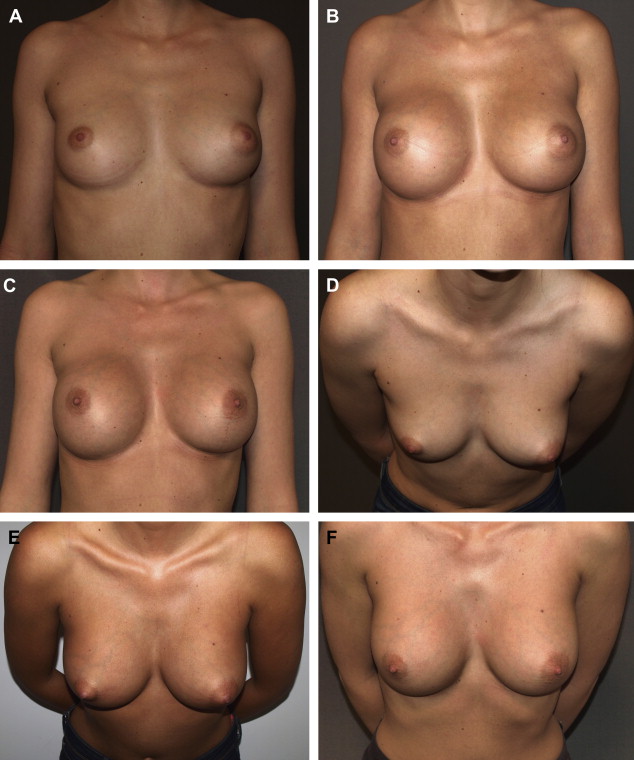
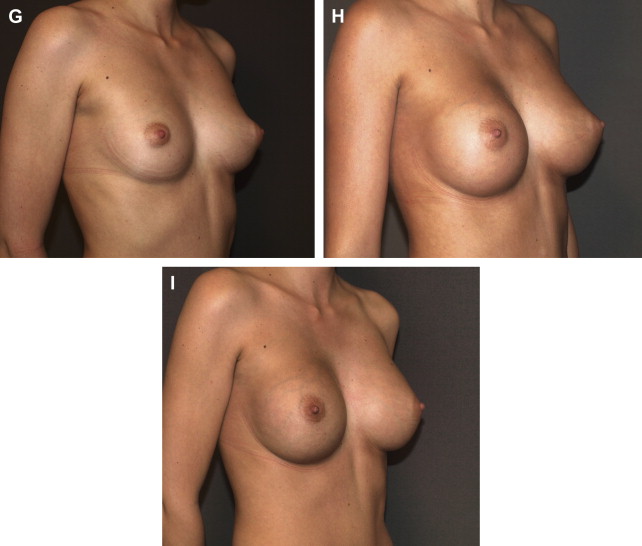
Simultaneous use of a breast implant and autologous fat grafting is a simple concept, which combines the benefits of effective breast augmentation provided by implants with the remodeling capabilities provided by fat. Even more importantly, this technique obviates retromuscular implant placement in thin patients who present with reduced skin flap thickness. The primary author commenced using this technique in 2006, initially in secondary cases to camouflage visible implants (Case 1; Fig. 1 ), followed soon by use in primary cases (Case 2; Fig. 2 ). Although the author published this technique in 2009, his group further published a series of clinical cases demonstrating the efficacy of this procedure in 2013, thus introducing the term “composite breast augmentation.”

Introduction or overview
For over 10 years, numerous investigators have described the successful and extensive use of fat grafting in plastic surgery. The original concept of fat micrografting can be attributed to Coleman. Through his work, liposculpture and its benefits were introduced, initially in the face, followed by grafting to the breast and body. The evolution of micrografting was further supported by the work of Yoshimura and colleagues in their sentinel article discussing cell-assisted lipotransfer for cosmetic breast augmentation. Throughout the history of fat grafting, concerns have been raised regarding its safety in postoperative surveillance of breast architecture. Such concerns have been addressed by Delay and colleagues who demonstrated that fat grafting does not in fact interfere with mammographic interpretation. Rubin and colleagues demonstrated that fat grafting of the breast produced fewer radiographic abnormalities and improved Breast Imaging Reporting and Data System (BI-RADS) scores with less-aggressive follow-up recommendations by breast radiologists when compared with reduction mammoplasty, a widely accepted procedure. Cameron and colleagues had comparable conclusions with their series of patients operated with the CBA technique. The significant contributions of Khouri and colleagues must also be recognized. In this article by Khouri and colleagues, they introduce the BRAVA device (Brava, LLC, a subsidiary of Bio-mecanica Inc, Miami, FL, USA), which, when used in combination with fat grafting, improves fat engraftment by enlarging the capacity of the recipient site and enhancing the vascularity of the breast.
Although this list is by no means exhaustive, it certainly demonstrates the pivotal role fat grafting has in modern plastic surgery and recognizes the numerous surgeons who have contributed to its evolution. Interest in fat transfer is not new, as well summarized by Mazzola elsewhere in this issue. However, it can be said that the first technical refinements made by Coleman, followed by many other contributors, have not only significantly improved the quality of results but also broadened the indications.
Simultaneous use of a breast implant and autologous fat grafting is a simple concept, which combines the benefits of effective breast augmentation provided by implants with the remodeling capabilities provided by fat. Even more importantly, this technique obviates retromuscular implant placement in thin patients who present with reduced skin flap thickness. The primary author commenced using this technique in 2006, initially in secondary cases to camouflage visible implants (Case 1; Fig. 1 ), followed soon by use in primary cases (Case 2; Fig. 2 ). Although the author published this technique in 2009, his group further published a series of clinical cases demonstrating the efficacy of this procedure in 2013, thus introducing the term “composite breast augmentation.”
Treatment goals and planned outcomes
In cases of primary breast augmentation, the aim of CBA is to provide appropriate coverage of the implant in patients who have reduced skin thickness in the presternal area ( Fig. 3 ). This coverage then obviates a submuscular pocket and its associated drawbacks (eg, pain and animation with activity). It is desirable to offer patients a single-stage surgery, with minimal downtime. In addition, the final result should appear natural and proportionate.
Related posts:
 Fat Grafting for Facial Filling and Regeneration
Primary Breast Augmentation with Fat Grafting
The Role of Fat Grafting in Breast Reconstruction
Regenerative Approach to Velopharyngeal Incompetence with Fat Grafting
Regenerative Approach to Scleroderma with Fat Grafting
Percutaneous Aponeurotomy and Lipofilling (PALF)
Fat Grafting for Facial Filling and Regeneration
Primary Breast Augmentation with Fat Grafting
The Role of Fat Grafting in Breast Reconstruction
Regenerative Approach to Velopharyngeal Incompetence with Fat Grafting
Regenerative Approach to Scleroderma with Fat Grafting
Percutaneous Aponeurotomy and Lipofilling (PALF)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


