Organ or site
Diagnostic (sufficient to establish the diagnosis of chronic GVHD)
Distinctive (seen in chronic GVHD, but insufficient alone to establish a diagnosis)
Other features or unclassified entities
Skin
Poikiloderma
Lichen planus–like features
Sclerotic features
Morphea-like features
Lichen sclerosus–like features
Depigmentation
Papulosquamous lesions
Sweat impairment
Ichthyosis
Keratosis pilaris
Hypopigmentation
Hyperpigmentation
Nails
Dystrophy
Longitudinal ridging, splitting, or brittle features
Onycholysis
Pterygium unguis
Nail loss (usually symmetric, affects most nails)
Scalp and body hair
New onset of scarring or nonscarring scalp alopecia (after recovery from chemoradiotherapy)
Loss of body hair
Scaling
Thinning scalp hair, typically patchy, coarse, or dull (nor explained by endocrine or other causes)
Premature gray hair
Table 7.2
Skin scoring of chronic graft-versus-host disease (cGVHD)
Score 0 | Score 1 | Score 2 | Score 3 | |
|---|---|---|---|---|
GVHD features to be scored by BSA: | No BSA involved | 1–18 % BSA | 19–50 % BSA | >50 % BSA |
Check all that apply: Maculopapular rash/erythema Lichen planus–like features Sclerotic features Papulosquamous lesions or ichthyosis Keratosis pilaris–like GVHD | ||||
Skin features score: Other skin GVHD features (NOT scored by BSA) Check all that apply: Hyperpigmentation Hypopigmentation Poikiloderma Severe or generalized pruritus Hair involvement Nail involvement | No sclerotic features | Superficial sclerotic features “Not hidebound” (able to pinch) | Check all that apply: Deep sclerotic features “Hidebound” (unable to pinch) Impaired mobility Ulceration | |
Abnormality present but explained entirely by non-GVHD documented cause (specify): _________________ | ||||
Nail changes, including dystrophy, longitudinal ridging, onycholysis, pterygium, and anychia (loss of the nail entirely) are also considered distinctive features [1]. Hair loss may be associated with cGVHD, but evaluating alopecia in the setting of HSCT is challenging, and the etiology is often multifactorial. Skin pathology can be helpful in determining the etiology and guiding the treatment.
The skin is the organ most commonly involved at the time of initial cGVHD diagnosis. The purpose of this chapter is to better acquaint the medical team with the nonsclerotic epidermal manifestations of cutaneous cGVHD, in the hope that early recognition and uniformity in grading of these clinical features will aid in diagnosis, treatment, and research.
Clinical Manifestations of cGVHD
Diagnostic Features
Diagnostic features for cGVHD (requiring no further testing to establish the presence of cutaneous cGVHD) include lichen planus–like lesions, lichen sclerosus, and poikilodermatous skin changes [1]. Each diagnostic feature may be seen alone, but they often appear in combination, along with other epidermal or sclerotic features of cutaneous GVHD.
Lichen Planus–like GVHD
Lichen planus is characterized by purple-hued, polygonal papules and plaques, sometimes with a fine white scale and an overlying network of white lines (Wickham striae). Lichen planus of the hair follicle is termed lichen planopilaris (Figs. 7.1, 7.2, 7.3, 7.4, 7.5, 7.6, 7.7, 7.8, 7.9, 7.10 and 7.11).

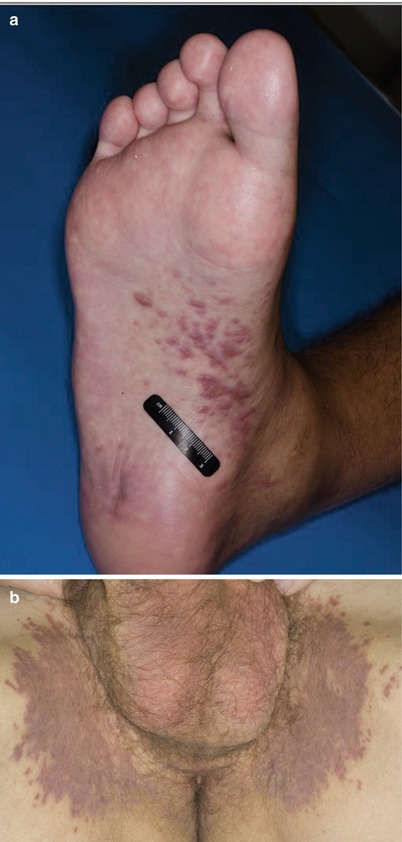
Fig. 7.1
The purple, polygonal lichen planus–like papules and plaques may be solitary (a, b) or may become confluent (c, d)
Fig. 7.2
(a, b) Lichen planus-like GVHD may koebnerize, following lines of pressure or trauma. (c) An unusual sporotrichoid pattern (arrows) is present without known antecedent. Trauma
Fig. 7.3
Inflammation may lead to significant postinflammatory pigment changes, including the hypopigmentation and hyperpigmentation seen in the beard area of this patient
Fig. 7.4
Unusual presentations of lichen planus–like GVHD may occur, including prominent lesions in distribution that may mimic tinea pedis (a) and tinea cruris (b). This patient had been treated with topical antifungal agents
Fig. 7.5
(a, b) Lichen planus–like GVHD may become hypertrophic, mimicking prurigo nodularis or squamous cell carcinoma
Fig. 7.6
 Grading and Treatment of Acute Graft-Versus-Host Disease
Grading and Treatment of Acute Graft-Versus-Host Disease
 Wound Care in the Management of Chronic Graft-Versus-Host Disease
Wound Care in the Management of Chronic Graft-Versus-Host Disease
 Clinical Presentation of Acute Cutaneous Graft-Versus-Host Disease
Clinical Presentation of Acute Cutaneous Graft-Versus-Host Disease
 Dermal and Subcutaneous Chronic Graft-Versus-Host Disease
Dermal and Subcutaneous Chronic Graft-Versus-Host Disease
 Diagnosis, Staging, and Treatment of Chronic Graft-Versus-Host Disease
Diagnosis, Staging, and Treatment of Chronic Graft-Versus-Host Disease
 Clinical Presentation of Nonsclerotic Epidermal Chronic Graft-Versus-Host Disease and Hair and Nail Changes
Clinical Presentation of Nonsclerotic Epidermal Chronic Graft-Versus-Host Disease and Hair and Nail Changes




Lichen planus–like changes may cause scarring. These scalp (a) and facial (b) lesions are difficult to distinguish from those of chronic cutaneous lupus
Related posts:
Grading and Treatment of Acute Graft-Versus-Host Disease
Wound Care in the Management of Chronic Graft-Versus-Host Disease
Clinical Presentation of Acute Cutaneous Graft-Versus-Host Disease
Dermal and Subcutaneous Chronic Graft-Versus-Host Disease
Diagnosis, Staging, and Treatment of Chronic Graft-Versus-Host Disease
Clinical Presentation of Nonsclerotic Epidermal Chronic Graft-Versus-Host Disease and Hair and Nail Changes
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
