Fig. 4.1
Ocular graft-versus-host disease. Ocular GVHD can affect almost every structure of the eye. Distinctive characteristics of chronic ocular GVHD include keratoconjunctivitis sicca, confluent areas of punctate keratopathy, and cicatricial conjunctivitis. (a) Acute ocular GVHD can present with pseudomembranous conjunctivitis and sloughing of the cornea, which can be visualized using fluorescein dye staining or slit lamp examination. (b) Complete loss of eyelashes may also be seen in the setting of acute ocular GVHD. (c) In chronic ocular GVHD, punctate keratopathy involving the cornea and conjunctiva can be seen in the setting of keratoconjunctivitis sicca, or dry eye syndrome, and can be visualized with the aid of dyes including fluorescein, lissamine green (as shown), and rose Bengal. (d) Blepharitis, or inflammation of the eyelids, may also be observed and can lead to trichiasis—ingrowth or misdirection of eyelashes, which can result in corneal abrasion. (e) Chronic inflammation of the ocular mucosa can lead to conjunctival fibrosis, which can be visualized with eyelid eversion (Photos courtesy of Manuel B. Datiles III, MD)
Fig. 4.2
Diagnostic and distinctive features of oral GVHD. Chronic GVHD may be clinically diagnosed by the presence of lichen planus–like hyperkeratosis on the oral mucosa in a patient who has undergone stem cell transplantation. (a) Chronic GVHD may present as white reticulate, hyperkeratotic plaques on the buccal mucosa. (b) Erythema, hyperkeratotic plaques, and pseudomembranous ulceration may be observed in chronic GVHD. Acute GVHD may have a similar ulcerated presentation with mild erythema and without hyperkeratotic plaques. (c) Mucocutaneous candidiasis, presenting here as white plaques on the posterior soft palate and anterior pillar of fauces (arrows) and yellow-coated tongue, can mimic acute or chronic GVHD but is generally accompanied by a burning sensation relieved with topical and systemic antifungal therapy
Fig. 4.3
Oral ulcerations in post-transplant patients. Ulcerations may occur at any site on the oral mucosa, including the roof of the mouth, buccal mucosa, tongue, gingiva, vestibules, and lips. Establishing a clear diagnosis is critical for successful treatment. Ulcers may result from GVHD, viral infection, systemic medications or other causes. (a) Acute GVHD may present as mucositis involving any site on the oral mucosa (Photo courtesy of Robert Range, DDS). (b, c) Pseudomembranous ulcerations in chronic GVHD occur in many forms, and may eventually lose their pseudomembranous covering. Common sites include the base of the ventral tongue and the buccal mucosa. (d) Chronic GVHD may present on the cutaneous lip as wide, irregularly shaped ulcers in the setting of white lacy lesions, chapping, or generalized superficial hyperkeratosis of the cutaneous lip. (e) Ulcerations on the cutaneous lip may also be caused by viruses, including herpes simplex virus (HSV). HSV presents as clustered vesicles that, when unroofed, leave punched-out ulcerations. (f) Sirolimus, and less frequently other mTOR inhibitors, may induce isolated painful oral ulcerations, mucositis, or stomatitis. These findings typically occur in the setting of supratherapeutic serum drug levels and resolve with adjustment of drug dose. Palliative care may be required to help reduce oral pain until resolution of the ulcers
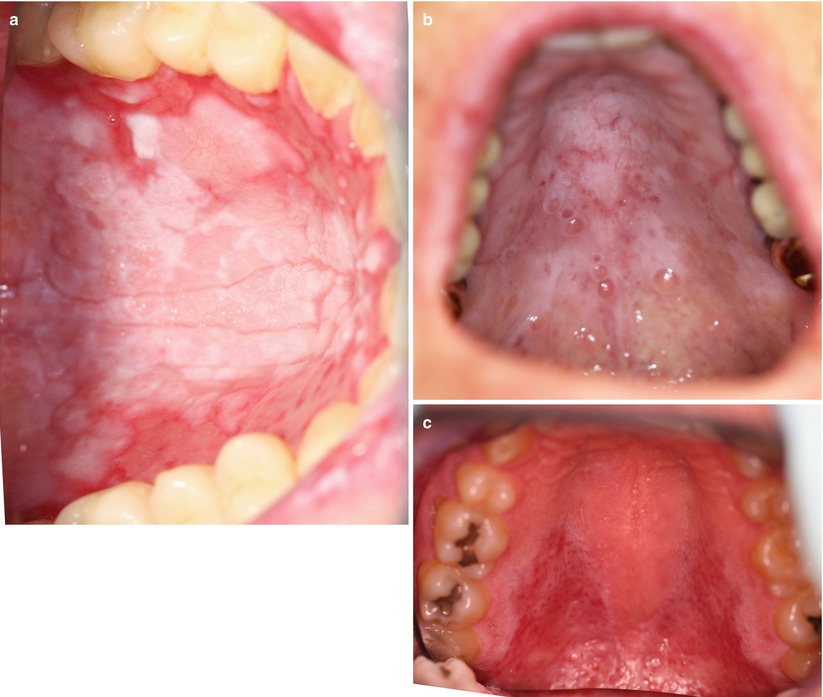
Fig. 4.4
Palatal changes in oral chronic GVHD. Alterations in the palatal mucosa may be seen in chronic GVHD. (a) Palatal hyperkeratosis, erythema, and ulceration may be present on the hard palate and soft palate in chronic GVHD. (b) The presence of mucoceles is a distinctive, but not diagnostic, sign of oral chronic GVHD. Mucoceles occur when the ductal openings of the minor salivary glands are blocked, either with foreign material or because of lymphocytic infiltrate in the underlying skin or salivary glands. These are most commonly seen on the lower labial mucosa and at the junction between the hard and soft palate. Though typically painless, mucoceles may be bothersome and slow to resolve. (c) Milder changes involving the palate, such as a mottled red and white discoloration, may also be seen in chronic GVHD

Fig. 4.5
Tongue changes in post-transplant patients. The tongue is a sensitive indicator of changes in the post-transplant period. In the setting of long-standing xerostomia or prolonged oral chronic GVHD, the tongue may lose its filiform and fungiform papillae, resulting in smooth appearance of the dorsal tongue. (a) When xerostomia is induced by chronic GVHD, associated white hyperkeratotic plaques may also be seen on the dorsal surface. (b) Hyperkeratotic plaques on the dorsal tongue may also be patchy and intermixed with patches of atrophy and erythema. (c) Chronic GVHD may induce isolated or multiple tufted, hyperkeratotic papules and plaques on the dorsal tongue, which require careful monitoring and evaluation with diagnostic biopsy to assess for human papillomavirus (HPV) or secondary malignancy
Fig. 4.6
Genital GVHD. Chronic GVHD of the genitals may manifest as erythema, white plaques, erosions, fissures, ulcerations, or significant scarring resulting in loss of normal genital anatomy if not diagnosed at an early stage. Symptoms include vaginal dryness, pruritus, dyspareunia, and pain to touch around the introitus, particularly concentrated at the Skene’s and Bartholin’s duct openings. Genital GVHD may occur alone, but typically is associated with involvement of other mucosal sites [1]. (a) Chronic lichen planus-like GVHD of the genital mucosa is characterized by reticulate leukokeratosis (Wickham striae) overlying erythematous patches or erosions and can lead to complete resorption of the labia minora (arrow), clitoral hood agglutination (arrowhead), and narrowing of the vaginal orifice (double arrowhead). The vagina should always be examined for involvement in all forms of GVHD. (b) Erosive GVHD is characterized by painful erosions and ulcerations favoring the modified mucous membranes of the labia minora, perineum, clitoral prepuce, vestibule, and vaginal mucosa. The resulting vaginal stenosis, synechiae, and labial adhesions often require surgical correction to maintain sexual and urinary function and to prevent hematocolpos [2]. (c) Lichen sclerosus–like GVHD is characterized by waxy, hypopigmented plaques (arrow) and loss of genital structures secondary to scarring. Agglutination of the labia minora (arrowhead) and clitoral hood scarring (double arrowhead) may be seen. (d) Male genital GVHD is not well characterized. Reported presentations include appearances resembling lichen planus (arrow) or lichen sclerosus, phimosis, meatal scarring [3], and Peyronie’s disease [4]. Coronal fusion (arrowhead) may also be seen
Table 4.1
Differential diagnosis of ocular graft-versus-host disease by clinical features
Xerophthalmia [5] | Conjunctival injection (“Red Eye”) [5] | |||
|---|---|---|---|---|
DDx | Drug-induceda Injury secondary to total body irradiation Infectionb Other medical conditionsc | Infectionb Trauma | Infectionb Glaucoma Allergy Chemical irritant Corneal abrasion Subconjunctival hemorrhage | Autoimmune diseases (ocular cicatricial pemphigoid) Postinfectious conjunctivitis Ocular rosacea Atopic keratoconjunctivitis |
Useful Tests | Schirmer tear test Tear film breakup time Meibomian gland exam Tear osmolarity measurement Corneal and/or conjunctival stainingd | Slit lamp examinatione Corneal and/or conjunctival stainingd Conjunctival or corneal sampling for microbiological evaluation | Slit lamp examinatione Measurement of intraocular pressure Corneal and/or conjunctival stainingd Conjunctival or corneal sampling for microbiological evaluation | Slit lamp examinatione Eversion of upper and lower lids Conjunctival or corneal sampling for microbiological evaluation Conjunctival biopsy ± direct immunofluorescence |
Table 4.2
Differential diagnosis of oral graft-versus-host disease by clinical features
Xerostomia | Oral erosions and ulcerations | Mucosal erythema | White patches and plaques | |
|---|---|---|---|---|
DDx | Drug-induced hyposalivationa Dehydration Injury secondary to total body irradiation | Drug-inducedb Viral infectionc | Gingivitis Erythematous candidiasis Irritant or allergic contact mucositis | Wipes away with gauze Candidiasis/thrush Pseudomembrane Fixed HPV-reactive hyperkeratotic plaque Leukoplakia Secondary malignancy (SCC) |
Useful tests | Increase patient liquid intake Review medication list for anticholinergic agents Palpate major salivary glands to observe saliva expression Minor labial salivary gland biopsy to assess for histopathologic features of GVHD Consider trial of cholinergic agonist drug | Assess plasma levels of offending drugb Viral direct fluorescent antibody, PCR and/or culture Incisional mucosal biopsy of affected, intact tissue adjacent to defect | Assess for local irritating factors (heavy dental calculus, poor oral hygiene) KOH preparation and fungal culture for Candida Incisional mucosal biopsy | KOH preparation and fungal culture for Candida Incisional mucosal biopsy |
Table 4.3
Differential diagnosis of genital graft-versus-host disease by clinical features
Vulvovaginal dryness [11] | Mucosal erythema [13] | White patches and plaques [13] | Vulvar pain and/or dyspareunia [14] | |||
|---|---|---|---|---|---|---|
DDx | Estrogen deficiency Drug- induceda | Viral infectionb Secondary malignancy Candidiasis Bacterial infection Sexually transmitted infections (STI)c Drug reactiond | Estrogen deficiency Erythematous candidiasis Bacterial infection Irritant or allergic contact dermatitis Vulvar intraepithelial neoplasia (VIN) Plasma cell mucositis | Lichen planuse Lichen sclerosuse Lichen simplex chronicus Vitiligo Postinflammatory pigment alteration Candidiasis Condyloma VIN/squamous cell carcinoma | Estrogen deficiency Vulvodyniae | Candidiasis Bacterial infectionf Trichomoniasis Atrophic vaginitis Vaginal intraepithelial neoplasia Vaginal condyloma Cervicitisg
Related posts: Grading and Treatment of Acute Graft-Versus-Host Disease Grading and Treatment of Acute Graft-Versus-Host Disease
 Wound Care in the Management of Chronic Graft-Versus-Host Disease Wound Care in the Management of Chronic Graft-Versus-Host Disease
 Clinical Presentation of Acute Cutaneous Graft-Versus-Host Disease Clinical Presentation of Acute Cutaneous Graft-Versus-Host Disease
 Dermal and Subcutaneous Chronic Graft-Versus-Host Disease Dermal and Subcutaneous Chronic Graft-Versus-Host Disease
 Diagnosis, Staging, and Treatment of Chronic Graft-Versus-Host Disease Diagnosis, Staging, and Treatment of Chronic Graft-Versus-Host Disease
 Clinical Presentation of Nonsclerotic Epidermal Chronic Graft-Versus-Host Disease and Hair and Nail Changes Clinical Presentation of Nonsclerotic Epidermal Chronic Graft-Versus-Host Disease and Hair and Nail Changes
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|