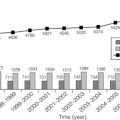
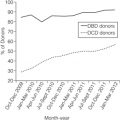
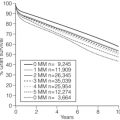
13 The development of CTD varies in each organ. Epithelial injury is the primary cell target in the kidney and lung, although more recent data have implicated microvascular injury as the target of both organs. In the heart, however, endothelial cells are the primary target of injury, which may be mediated by both immune- and non-immune-dependent phenomena.1 Immune-mediated injury may occur by cellular- and/or antibody-mediated pathways, the latter becoming more frequently recognised in all solid organs with our expanded understanding of the humoral immune response. Due to the differences in allograft injuries, we will discuss each organ separately and compare the presentations and outcomes when relevant. In cardiac allografts, CTD is a disorder manifested by clinical dysfunction and accelerated cardiac allograft arteriosclerosis, known as cardiac allograft vasculopathy (CAV). CAV is extremely common, seen in ~ 7% of recipients at 1 year, 32% at 5 years and in more than half at 10 years post-transplant.2 CAV and late graft failure (i.e. unrecognised CAV) account for about 31% of deaths at 5 years post-transplant. Risk factors include the more traditional associations with hypertension, diabetes and dyslipidaemia, with transplant-related risks that include cytomegalovirus (CMV) infection, donor cause of death, number of human leucocyte antigen (HLA) mismatches between donor and recipient and the number of allograft rejection episodes.3 The pathognomonic lesion of CAV is concentric intimal thickening affecting the coronary vessels, particularly the smaller distal intramyocardial vessels. Myocardial fibrosis may also be seen in some cases. However, until recently, there were disparate definitions of CAV based on the histology, angiographic findings and findings on intravascular ultrasound. In 2010, the International Society of Heart and Lung Transplantation (ISHLT) published guidelines for the terminology of cardiac allograft vasculopathy with the goal of having a more universal and prognostically significant definition that would also serve as an end-point of clinical trials. The consensus of the ISHLT working group was to base the definition and diagnosis of CAV on conventional invasive coronary angiography. A grading system based on angiographic findings and graft function (evaluated by echocardiography or invasive haemodynamic data) was established (Box 13.1).4 This new definition was based on evidence from a large population study performed by Costanzo et al., in which 4637 postoperative angiograms were performed to look for CAV. The study demonstrated an overall likelihood of death or re-transplantation secondary to CAV of 7%, and 50% of patients with severe disease are likely to reach that outcome.5 According to the guidelines, there is no role of routine intravascular ultrasound (IVUS) surveillance or non-invasive computed tomography (CT)-based angiography for assessment of CAV. Immune-based markers, gene-based and protein-based biomarkers (B-type natriuretic peptide, cardiac-specific troponins, high-sensitivity C-reactive protein), microvascular function testing and stress-based imaging were not recommended for inclusion in the above nomenclature algorithm as markers for defining severity of CAV due to lack of standardisation. While much focus has been placed on cellular immunity mediating this disorder, the demonstration of endothelial injury as a key feature has led to a renewed interest in anti-donor antibodies and antibody-mediated rejection (AMR). A considerable hurdle has been the lack of uniform diagnostic criteria for AMR in heart allografts. The histological criteria have recently been standardised and consensus obtained.6 The Consensus Conference on Antibody Mediated Injury in Heart Transplantation performed a thorough review of the diagnostic and clinical considerations, recognising the strong relationship between AMR, CAV and recipient death.7 Importantly, it was established that the detection of antibody within the allograft, even in the absence of cardiac dysfunction, is associated with a greater mortality and more likely development of CAV. The recognised spectrum of cardiac AMR includes a latent phase in which circulating antibody may be present, followed by a silent phase of deposition in the allograft without histological or clinical alterations, and progression to a subclinical phase with circulating antibody and histology, and finally symptomatic disease. This paradigm may be similar in other solid-organ injuries where antibody plays a role in the development of allograft failure. Recently, antibodies against the major histocompatibility class I-related chains A (MICA) and B (MICB), polymorphic cell surface proteins expressed by a wide variety of human cells including epithelial cells, endothelial cells and monocytes, have been associated with CAV. Current reports are inconclusive as to whether these antibodies to MICA and MICB are directly detrimental or whether they are biomarkers of high immunological risk recipients.8,9 Recommendations have been made for screening for donor-specific antibody (DSA) as well as timing for surveillance allograft biopsies on a serial basis. It is clear, however, that additional studies are needed to determine not only the most effective therapeutic interventions to minimise long-term CTD, but also to determine the effect of prophylactic therapy.7 Unlike the other solid organs, the liver may enjoy prolonged allograft survival, even with minimisation of immunosuppression. The contribution of cellular rejection episodes to long-term graft failure is lessened, perhaps in part due to the liver’s tolerogenic capabilities.10 Moreover, complications of immunosuppression such as nephrotoxicity and malignancy have a greater impact on recipient outcome. Similarly, recurrent disease is a key contributor to late graft failure and the development of newer therapies for hepatitis C may have a critical impact on the mortality and re-transplantation needs in this field. Thus significant efforts have been expended in the liver to identify those recipients that may be suitable candidates for immunosuppressive withdrawal as well as to identify more effective strategies to manage immunosuppression.11 Because these studies are beyond the scope of this chapter, the reader is referred to other reviews on this topic. Chronic allograft rejection, while a less common cause of late graft failure, is a recognised entity that is defined as an immunological injury to the allograft, usually as a result of persistent and unrelenting acute rejection, and results in irreversible damage to the bile ducts, veins and arteries.12 The onset is months to years post-transplant and graft failure may occur within a year of transplantation. This may occur in about 3–5% of recipients, and risk factors include both immune-dependent and immune-independent factors. In the former, this includes the frequency and severity of acute cellular rejections, lower baseline immunosuppression and primary immune disease diagnosis; in the latter, risk factors are non-Caucasian race, younger recipient age and donor age greater than 40. A critical component to diagnosis is histology, which is more complex than previously appreciated. Late allograft biopsy is typically performed due to abnormalities in routine lab testing for liver function. The use of terms such as ‘vanishing bile duct syndrome’ or ‘ductopenic rejection’ is no longer recommended, as bile duct loss is just one component of graft failure. Native disease recurrence is a critical issue, as already noted, and may confuse diagnostic interpretation.13 These diagnoses include: 1. Infectious aetiologies (viral hepatitis A, B, C, D). 2. Dysregulated immunity (autoimmune hepatitis, primary biliary cirrhosis, primary sclerosing cholangitis, sarcoidosis). 4. Toxicities (alcohol, drugs). 5. Metabolic disorders (including non-alcoholic steatohepatosis). The minimum diagnostic criteria for chronic rejection are listed in Table 13.1.12 Biopsies often include non-specific changes such as portal-based chronic inflammation. Interpretation should include an assessment of the adequacy (survey of at least six portal tracts), systematic examination of the tissue and through clinical correlation. Until recently, standard criteria have not been utilised and based on centre expertise. Thus, consensus criteria for common causes of late allograft failure have been developed and are discussed in depth.13 This more structured analysis provides uniformity in diagnosis and highlights the common similarities in some disease features. Table 13.1 Banff criteria for liver allograft chronic rejection (CR) Reproduced from Demetris A, Adams D, Bellamy C et al. Update of the International Banff Schema for Liver Allograft Rejection: working recommendations for the histopathologic staging and reporting of chronic rejection. An International Panel. Hepatology 2000; 31(3):792–9. Bronchiolitis obliterans syndrome (BOS) is a major factor limiting long-term graft survival and is the clinical manifestation of CTD in the lung. Despite the potency of immunosuppression, BOS remains a difficult issue and nearly half of all lungs transplanted will develop this by 5 years after transplantation.14 Once diagnosed, only 30–40% of recipients with BOS survive to 5 years and beyond its onset. Detection and grading of this disorder is primarily by measuring forced expiratory volume in 1 second (FEV1) as opposed to histological or radiological findings (Table 13.2).15 Table 13.2 Proposed classifications of BOS In 2001, a new classification system of BOS was proposed which included FEF25–75 (mid-expiratory flow rate) to recognise early airflow obstruction (Table 13.2).15 Other contributory factors that affect FEV1 should be excluded, such as acute rejection, infection, excessive recipient weight gain, anastomotic dysfunction, respiratory muscle dysfunction and other technical problems. Immune-dependent risk factors for the development include degree of HLA mismatch, acute rejection episodes and autoimmune reactions to lung matrix components. Other antigen-independent factors include infections, gastro-oesophageal reflux, donor factors such as cigarette use, head injury as a cause of death, airway ischaemia and inhaled irritants.16 In BOS there is epithelial injury, mediated predominantly by cellular immune responses, although more recent data indicate both allo- and autoantibodies may contribute to injury.16 Inflammation is associated with progressive airway damage and fibrosis, with eventual bronchial scarring and obstruction. Transbronchial biopsy histology may reveal inflammation and fibrosis of the cartilaginous airways and particularly within the smaller airways, with inflammation and fibrosis in the lamina propria and luminal surfaces of bronchioles, while larger bronchi may show peribronchial fibrosis and bronchiectasis. Surrounding alveoli and interstitium may appear normal. Antibodies against non-HLA graft proteins have been associated with late graft failure in the lung. Analysis of serial serum samples from recipients with BOS has identified non-HLA antibodies in five of 16 recipients with BOS compared to none of the 11 without BOS.17 The specificity of this anti-airway epithelial cell antibody is under investigation, but is associated with up-regulation of transforming growth factor (TGF)-β signalling in vitro. Complement activation is also seen in BOS biopsies, associated with anti-endothelial cell antibodies. Immune responses against collagen V epitopes have also been implicated in the pathology of graft failure in BOS. Management of these patients is complex. Intensification of immunosuppression may be needed if acute rejection is a key contributor, but in the setting of infection this may be ineffective and in fact harmful to infection clearance. A number of approaches have been attempted but there is no uniformly accepted management, and most are not highly effective.18 Further investigation into the mechanisms of injury using preclinical models as well as human trials is a clear priority for this field. Pancreas transplantation for type I diabetes mellitus has seen substantial improvements in success both in terms of patient and allograft survival. Graft survival varies based on whether transplantation is simultaneous with the kidney, with 10-year survival of 54% compared to only 27% in solitary pancreas transplantation.19 CTD of the pancreas is known as chronic rejection. While the emphasis in the past has been on alloimmune injury to mediate chronic rejection, accumulating data suggest that recurrent autoimmune responses to islets may be a key contributor to graft loss, despite the use of potent immunosuppression.20 Graft deterioration is associated with hyperglycaemia, although this is a non-specific finding and may also be seen in insulin resistance and beta-cell loss associated with tacrolimus therapy. Serum pancreatic enzyme elevations are similarly of limited value due to the lack of specificity. Loss of insulin expression following glucose or arginine stimulation or a decline and loss of C-peptide may also be seen, but when detected indicate irreversible loss of beta-cell function and, again, are non-specific findings. Thus there is no specific biomarker of CTD and allograft biopsy remains the primary technique to assess the aetiology of graft dysfunction. Histological features include septal (perivascular) fibrosis with mononuclear cell inflammation and progressive acinar loss. Vascular changes such as narrowing of arterial lumina and concentric fibroproliferative endarteritis are considered an integral part of the pattern of CTD. The extent of acinar inflammation during acute rejection episodes is recognised as a prognostic factor for the development of chronic rejection. Recently, standardised scoring was established by consensus at the Banff Meeting in 2007 (see Box 13.2) and provides a reproducible and reliable tool for assessing chronic rejection in allograft biopsies.21 These criteria, based on data accrued from experienced pancreas transplant centres, suggest that biopsy may contribute useful information to patient and graft management. Therapeutic interventions have focused on glucose control and immunosuppression, and the latter may be ineffective due to the late detection of disease. Further investigations are needed in this area as well as the consideration of non-calcineurin therapies to ameliorate the contribution of islet toxicity for late graft failure. Even in this era of potent immunosuppression with superb short-term graft survival and minimal levels of acute rejection in the first 6 months of transplantation, progressive graft loss of the kidney remains a considerable issue.22 Graft failure culminating in relisting for transplantation accounts for about 25–30% patients on the transplant waiting list. About half of kidney transplants are lost due to recipient death with a functioning graft due to cardiovascular disease, infection or malignancy. The remaining graft losses are due to failing function. In these recipients, chronic graft injury (CGI) is characterised by declining renal function with the histological features of progressive interstitial fibrosis and tubular atrophy (IF/TA), occurring months to years after transplantation, that may be accompanied by vascular and glomerular damage.1 In the past, clinicians have described this disorder using various terms such as chronic allograft nephropathy (CAN)23 and chronic rejection (CR). While these terms related to the characteristic histological features of IF/TA, they became a disease entity unto themselves and were used as a cause of late graft failure even in the absence of tissue for histological diagnosis. Consequently, in current clinical practice, the term ‘CAN’ has been eliminated and specific pathological investigations into the causes of IF/TA and functional failure are emphasised.24 The classification of chronic changes in kidney allografts was created in the Banff pathology meetings in the 1993–95 conferences and was revised in 2005 (Box 13.3). More recent studies suggest that failing allografts have identifiable diagnoses for injury, suggesting specific treatments may be available to ameliorate declining function, discussed in more detail below. Adoption of serial protocol biopsies and newer laboratory techniques (C4d staining, molecular profiling and solid-phase antibody assays) has led to a better understanding into causes of CGI, and emphasises the role of the humoral immune response. Indeed, the assessment of kidney graft pathology was formed by consensus at the Banff Meeting in 2005 and emphasised new criteria to assess for antibody-mediated injury, discussed below.24 IF/TA results as sequelae to a series of pathological insults to the kidney from the time of organ retrieval, which leads to incremental and cumulative damage to nephrons, and ultimate loss of graft function. Recent data from a number of studies now indicate that immune-mediated injury, especially related to alloantibodies, is a major threat to allografts even after the first year. In the recent cross-sectional analysis of failing kidney allografts from seven transplant centres in North America (the Deterioration of Kidney Allograft Function (DeKAF) study), the presence of IF/TA changes alone did not predict graft failure and allografts labelled as calcineurin inhibitor (CNI) toxicity fared no worse than other grafts in the absence of this diagnosis.25 The preponderance of abnormalities in this study featured immunological injury including acute rejection26 and antibody-mediated injury, occurring in about 57% of biopsies.27 Moreover, the presence of inflammation in the allograft, in areas of fibrosis and tubular atrophy that are not included in the Banff analysis of chronic injury, was an independent negative feature of allograft failure.28 Thus IF/TA is not an idiopathic and independent feature of a large proportion of failing allografts but identification of coincident pathology is important in defining outcome. Additional single-centre data were published by El-Zoghby et al.29 Three hundred and thirty kidney grafts were lost in 1317 conventional kidney recipients over a 10-year period. One hundred and fifty-three or 46% were lost due to graft failure. The causes of graft loss included glomerular disease such as recurrent disease, transplant glomerulopathy and de novo disease in 37%, acute rejection in 16%, other medical/surgical conditions in 16% and IF/TA in 31% of failed grafts. In this last group, an aetiology for IF/TA could be identified 81% of the time and CNI toxicity was rarely the cause, in only 0.7%, of failed allograft biopsies. These results demonstrate that glomerular damage is the most common cause of graft failure, as well as the paucity of true diagnoses of CNI toxicity. With the enhanced capabilities to detect donor-specific antibody, it is not unexpected that diagnoses of antibody-mediated injury are more common. This includes the utilisation of C4d staining and consensus about grading and histological features of injury.24,30,31 Moreover, there is now evidence that molecular analysis of allograft biopsies, even in the absence of diagnostic criteria for antibody-mediated rejection, may demonstrate endothelial cell activation indicative of active antibody-mediated damage and graft failure in patients with alloantibodies.32 These and many other observational studies have led us to think that late graft loss is not always a result of CNI nephrotoxicity and emphasises the need to investigate the cause of IF/TA. In understanding the development of CGI, a common paradigm is to classify these factors based on those that are antigen dependent (immunological) and those that are antigen independent (non-immunological). Note that this is an artificial partition and that non-immunological factors may ultimately mediate an immune response (Box 13.4). • Peri-transplant factors. These include: donor factors of age, donor serum creatinine and comorbid conditions such as hypertension; brain stem death with the accompanying catecholamine storm; preservation and implantation injury, e.g. ischaemic damage and reperfusion injury, leading to delayed graft function. • Post-transplant factors. These include immune response of acute rejection, both cellular and antibody mediated, and infections that may include urinary tract infection, donor derived infections and viral illnesses. Over time, recipient factors such as hypertension, dyslipidaemia, diabetes and viral infections, such as CMV and BK polyomavirus, play a more significant role in mediating renal tubular injury. In the past decade immunosuppression with CNIs was considered to be a significant contributor to late histological changes and allograft dysfunction; however, that paradigm has shifted, with evidence mounting in support of alloimmune injury being a major contributor of CGI. Donor age has a significant impact on graft survival and extremes of age are associated with worse long-term graft survival. With ageing, there is a reduction in nephron mass. Moreover, the ageing donor has attendant issues that affect long-term function. The concept of cellular senescence may limit the healing process in an organ allograft, due to a finite healing response in ageing tissue.33 Additionally, recipient-based stresses such as hypertension and diabetes may similarly be poorly tolerated. Donation after brain stem death is also significantly associated with worse graft survival and increased incidences of delayed graft function and acute rejection compared to live donor organs. The systemic sequelae of brain death are not well understood and direct injury to the brain stem may result in labile blood pressure, alterations in thermal regulation, endocrine and biochemical derangements, and alterations in renal function. Surges in catecholamine release are experienced, with resultant physical and structural changes affecting the vital organs. It may also be the trigger for the systemic release of proinflammatory mediators, resulting in endothelial cell activation and thrombotic microangiopathy. These processes enhance the immunogenicity of the organ. Delayed graft function (DGF) is a form of acute kidney injury seen following kidney transplantation, and may be defined as the need for dialysis support in the first 7 days post-transplantation. DGF incidence is rising, from 15% in 1985–1990 to 23% in 1998–2004,34 based on data from the United States Renal Data System. This may be related to the rising use of expanded criteria donors (ECDs), and the use of donors after declaration of circulatory death (DCD). DGF is a considerable issue, with an estimated increase of 41% for graft failure in those with DGF as well as a higher rate of rejection of nearly 40%, compared to recipients without DGF. There is also a strong association with the development of CTD, although non-biopsy proven. This complex series of injuries is significantly detrimental to long-term success and has led to a substantial interest not only in donor management, but also in therapeutic strategies to ameliorate ischaemic injury.35 Other strategies for improving outcomes include the use of perfusion of the kidney allograft; many centres have utilised this approach based on recent data demonstrating improved outcomes following pumping. Another opportunity may be graft protection through ‘immuno-cloaking’; that is, blocking the preserved allograft from further immune injury and allowing appropriate reparative processes to occur unimpeded.36 Finally, the kidney uniquely expresses TLR4 in mesangial cells, podocytes and tubular epithelium. As such, it is a focus of innate immune activation that triggers adaptive responses. Further therapies that may address this mechanism have potential to impact on DGF and thus CGI. The low incidence of CGI in grafts from HLA-identical living-related donors supports the role for immunological factors in developing CGI. Indeed, there has been a long-standing recognised association between acute rejection and CGI. However, early rejection episodes in the first 6 months do not necessarily portend worse graft survival, while later graft rejection episodes from 6 to 12 months or repeated episodes are associated with a significantly higher risk of graft loss. Importantly, if there is complete functional recovery with a late rejection episode, graft half-life is similar to recipients with no or early rejection episodes with impaired function.37 A complicating feature of these late graft rejections may be the superimposed presence of antibody-mediated rejection (AMR). Indeed, many of the data in this context were from an era when AMR was not recognised in its presentation beyond the early acute setting and may thus indicate a continuum of injury that contributes to CGI. While the association of donor-specific antibodies with late graft failure has long been recognised, it has not been until the last decade that the negative impact of donor-specific antibodies has been recognised as a predictor of graft loss. Alloantibody has been correlated to chronic rejection and graft dysfunction. In a prospective multicentre trial of 2278 recipients, 500 recipients had HLA antibodies. In these recipients, 6.6% of grafts failed compared to 3.3% among the 1778 patients without antibodies; 8.6% of grafts failed in patients who made de novo antibodies as compared to 3.0% in patients who did not make any antibodies, showing a higher rate of graft failure in patients with HLA antibodies.38 There are multiple studies correlating the development of donor-specific antibody (DSA) with allograft failure.39 In 1993, Feucht et al. for the first time identified C4d as a marker of kidney injury and chronic rejection in human kidney allograft biopsies. Numerous studies have reported the association of presence of C4d positivity on the biopsy specimen with chronic rejection and graft failure. Thus, acute AMR is defined histologically by the features in Box 13.5.40 Note that in the absence of detection of DSA, the diagnosis may be annotated as suspicious for AMR. Note that the presence of graft dysfunction is not required. The routine use of biopsy staining for C4d has led to an increased acceptance of the role of antibody-mediated damage in CGI and biopsy criteria have been defined.24 In 2005, criteria for chronic AMR were added to the Banff criteria for AMR. These criteria include: 1. Biopsy features including transplant glomerulopathy (TG; duplication or ‘double contours’ in glomerular basement membranes) and/or peritubular capillary basement membrane multilayering, and/or IF/TA with or without PTC loss, and/or fibrous intimal thickening in arteries without duplication of the internal elastica. 2. Diffuse C4d deposition in PTC. Note that if only either C4d deposits (with no DSA) or DSA (with no C4d) are present, with documented morphological capillary changes, then the diagnosis of ‘suggestive of chronic AMR’ is made.
Chronic transplant dysfunction
Organ-specific findings
Heart
Liver
Structure
Early CR
Late CR
Small bile ducts (< 60 mm)
Degenerative changes involving a majority of ducts: eosinophilic transformation of the cytoplasm; increased nuclear hyperchromasia; uneven nuclear spacing; ducts only partially lined by biliary epithelial cells
Degenerative changes in the remaining bile ducts
Loss in ≥ 50% of portal tracts
Terminal hepatic venules and zone 3 hepatocytes
Intimal/luminal inflammation
Lytic zone 3 necrosis and inflammation
Mild perivenular fibrosis
Focal obliteration
Variable inflammation
Severe (bridging) fibrosis
Portal tract hepatic arterioles
Occasional loss involving < 25% of portal tracts
Loss involving > 25% of portal tracts
Other
So-called ‘transition’ hepatitis with spotty necrosis of hepatocytes
Sinusoidal foam cell accumulation; marked cholestasis
Large perihilar hepatic artery branches
Intimal inflammation, focal foam cell deposition without luminal compromise
Luminal narrowing by subintimal foam cells
Fibrointimal proliferation
Large perihilar bile ducts
Inflammation damage and focal foam cell deposition
Mural fibrosis
Lung
Grade
Finding/severity
BOS 0
FEV1 > 90% of baseline
and FEF25–75 > 75% of baseline
BOS 0-p
FEV1 81–90% of baseline
and/or FEF25–75 ≤ 75% of baseline
BOS 1
FEV1 66–80% of baseline
BOS 2
FEV1 51–65% of baseline
BOS 3
FEV1 50% or less of baseline

Management
Pancreas
Kidney

Why and how does IF/TA occur? Clinical insights
The aetiology of chronic graft injury
Peri-transplant factors: beyond our control?
Post-transplant immunity: acute rejection
Post-transplant immunity: antibody-mediated rejection
Diagnosis of antibody-mediated rejection: acute and chronic

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Chronic transplant dysfunction
Only gold members can continue reading. Log In or Register to continue