Summary
The chin is a prominent aesthetic subunit.
Its reconstruction is complicated by the fact that it is a prominent convexity with little inherent laxity and little surrounding laxity.
It has functional significance supporting the lower lip, meaning poor reconstruction will result in oral incompetence.
17.1 Algorithm for Closure
The chin is quite frequently involved with Mohs resection for skin cancer (▶ Fig. 17.1). It is a prominent aesthetic unit with somewhat thick and oily skin that does not lend itself to grafting. Additionally, the convexity acts much like the vertex of the scalp with little surrounding laxity. The soft-tissue components of the chin are deeply adherent to the underlying mandible and there is little inherent tissue laxity for closure. The natural reservoir of laxity unfortunately comes from the lower lip and any excessive recruitment of lower lip tissue to reconstruct the chin will provide both a jarring postoperative appearance and external ectropion and subsequent oral incompetence. Fortunately, the chin tolerates tension on closure very well and the vast majority of chin defects can be managed appropriately by primary closure.
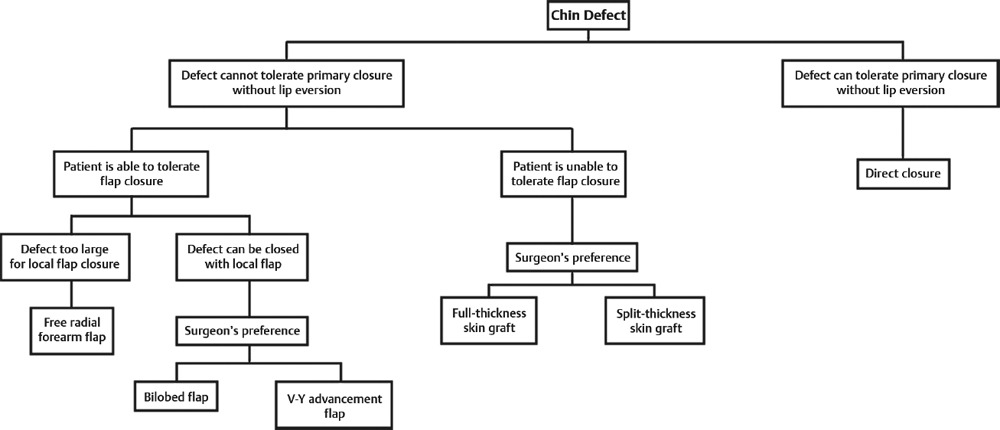
Fig. 17.1 Algorithm for chin defect closure.
17.2 Commonly Applied Methods of Closure
Primary closure with meticulous care for standing cones to avoid contour deformity and to avoid lower lip ectropion.
Bilobed flap reconstruction with recruitment from laxity of the neck and avoidance of excessive tension on the lower lip.
V-Y advancement flap.
Full-thickness skin grafts.
17.2.1 Primary Closure
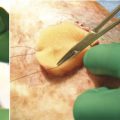
Primary closure involving the chin can be determined intraoperatively with a 2–0 Vicryl tacking suture placed vertically with planned dog-ear excisions superiorly and inferiorly. Even with significant tension on closure, with a sequential layered closure of 2–0 and 3–0 Vicryl, followed by interrupted 5–0 nylon sutures, the final aesthetic result is nearly always uniformly good to excellent. There is little need for undermining as simple advancement and closure under slight tension is more than adequate. At the time of closure, dog-ears need to be meticulously managed so that there is no contour deformity as this will rarely settle.
Early postoperative management including silicone sheeting and dermabrasion at 6-week intervals helps optimize the final scar 1, 2 (▶ Fig. 17.2 and ▶ Fig. 17.3).

Fig. 17.2 A 45-year-old female status post Mohs excision for basal cell carcinoma. Wound was closed with primary closure. Postoperative results shown at 4 months.

Fig. 17.3 A 52-year-old female status post 4 × 2 cm Mohs excision of recurrent melanoma in situ at left chin. Wound was closed with vertical primary adjacent tissue transfer with dog-ear excision. Postoperative results shown at 6 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


