- •
Surgical techniques can only indirectly improve textural changes of aging, particularly in difficult areas such as the perioral region.
- •
Standard approaches such as the Baker-Gordon peel and laser resurfacing can be effective but carry the danger of hypopigmentation and demarcation at the mandibular border.
- •
Although the Baker-Gordon peel is categorized as a ‘phenol’ peel, the active peeling agent is actually croton oil at a concentration of 2.1%. This high concentration is responsible for the results as well as the drawbacks.
- •
In the modern croton oil peel, the concentration is lowered, resulting in an effective and very versatile formulation, which can be used on all ages and skin types.
- •
The key to the modern peel is that the croton oil concentration is weak enough so that the method of application can be altered to determine the depth reached. This allows the surgeon precise control of the process.
- •
Different croton oil concentrations can be used in different areas of the face depending on relative skin thickness and clinical need.
Aging changes of the face can be broadly categorized into structural or gravitational changes, volumetric changes, and textural changes. There are many surgical procedures to deal with the first two, but surgery alone only indirectly improves textural issues and has no appreciable effect on perioral wrinkles or deep crow’s feet. Many patients view these textural changes to be equally or more important than structural changes and many an excellent facelift has been marred by persistent wrinkles in these difficult areas.
Previous techniques available, including the Baker-Gordon peel and CO 2 laser resurfacing, although effective, were attended by predictable and persistent hypopigmentation, leaving the skin with an alabaster, ghostly quality. These patients needed to accept the constant use of makeup, therefore this peel was limited to older, light-eyed individuals with pronounced wrinkling.
CO 2 laser resurfacing was touted as a significant improvement, but hypopigmentation, a long recovery, and prolonged erythema remained significant issues. The reputed advantage is the precision of the laser, but the reality is that enthusiasm for laser resurfacing is waning and recent reports have questioned the longevity of results with CO 2 laser resurfacing. There are now a multitude of gentler lasers such as Erbium and non-ablative technologies, but their cost effectiveness for well-established wrinkles remains questionable.
The use of modern croton oil peels became feasible as a result of the work of Gregory Hetter. Hetter studied the individual elements of the Baker-Gordon peel and questioned some of the beliefs that had been accepted without challenge for decades. He demonstrated that a weaker concentration of phenol did not penetrate deeper, and that croton oil (and not phenol) was the important peeling agent. An analysis of the Baker-Gordon formula revealed that the croton oil concentration was very high at 2.1%, responsible for both the notable results as well as the limiting problems. With this information at hand, the phenol concentration could be lowered and the concentration of the croton oil varied. By avoiding a problematic concentration of croton oil, this peel can be successfully utilized on all ages and skin types.
The key to the modern peel is that the croton oil concentration used is weak enough so that altering the application technique will affect the depth of peel. The intimidating ‘all or none’ quality of the Baker-Gordon peel was due to the very high croton-oil concentration which immediately resulted in dense frosting. The only option was a deep peel and the inevitable hypopigmentation. The advantage of the modern peel is that the surgeon can choose the depth of the peel by varying the concentration of croton oil depending on skin type, age, and clinical need. Since the croton oil concentrations are weaker, application technique is also a determinant of depth reached, allowing the surgeon to be in control of the entire process.
The indication for this peel is a desire to improve the texture of the skin, improve longstanding actinic changes, and rejuvenate the skin in a way that surgery is unable to do. It is now possible to achieve true clinical improvement without reaching a depth which results in hypopigmentation or an unnatural appearance. Moreover, different concentrations can be used in different parts of the face depending on skin thickness and degree of involvement. This degree of latitude allows successful peeling of delicate skin such as the eyelids and neck.
Operative technique
Pre-peel preparation
Adequate preparation prior to the peel is important to its success. Emphasis is placed on the post-peel phase so patients will be well informed as to what to expect. Photographs of the day by day recovery are routinely shown, and an effort is made for patients to speak or meet with individuals who have undergone a similar peel. Seeing someone who has had a good result is a powerful tool to show that the difficult early days are well worth the final result. Patients who are well informed tolerate the procedure well.
Prevention of pigmentary changes is an important part of the preparation and this is accomplished by using aggressive doses of tretinoin, hydroquinone, phytic acid or glycolic acid. The main ingredients are tretinoin and hydroquinone 4%, but use of the complete Obagi Nu-Derm system (Skin Specialists PC, Omaha, NE) in the preparation is valuable. The result is to stimulate the epidermis, stimulate the dermis to increase collagen content, and suppression of melanocytes. The purpose is to regulate cell function and reduce the risk of pigment alteration.
The process begins 4–6 weeks prior to peeling with tretinoin 0.1%, 1 inch (=1 g) applied over the whole face daily. This should extend to the earlobes, tragus, hairline and to one inch below the mandibular border and 1–2 mm below the lower ciliary edge. Avoid the upper lids as this can cause irritation. If the neck is to be peeled, the same preparation is used, decreasing the frequency if irritation results. Hydroquinone 4% is applied twice daily. The aim is to suppress and regulate melanocytes in an attempt to prevent post-inflammatory hyperpigmentation. Glycolic acid 8% or phytic acid 2% is used daily to accelerate exfoliation of desquamated cells in the stratum corneum.
This regimen is irritating and results in erythematous, flaky skin which the patient must accept. This preparation is stopped 4–5 days prior to the peel to allow settling of the epidermis. Although there is some controversy as to necessity of this regimen, skin prepared in this manner has been shown to respond better to deep peeling. In the author’s experience, skipping or shortening the preparation has resulted in a longer period of post-operative erythema.
Medications
Antiviral prophylaxis is used to prevent a herpetic outbreak. Valcyclovir hydrochloride 500 mg two times per day is begun 3 days prior to the procedure and continued for 1 week after peeling. Narcotic pain medication is routinely prescribed although the recovery is not particularly painful. Ibuprofen 800 mg three times per day is commonly used along with a Medrol Dosepak (Mova Pharmaceutical, Marrati, PR) beginning the day after the peel. The recovery is described as more of a nuisance, therefore sleep medication is prescribed.
Preparation of the solution
One of the advantages of the modern croton oil peels is that multiple solutions of different concentration and individual variations are easily mixed, even at a moment’s notice, resulting in impressive versatility. Preparation of the solution is a very important step that should be done by the operating surgeon or entrusted to someone else only if they are intimately acquainted with the process.
The ingredients are readily available, inexpensive, and the same as in the classic Baker-Gordon peel, including water, phenol, croton oil, and Septisol (Delasco, Council Bluffs, IA). Old formulations used drops of croton oil, which was cumbersome and could lead to variability due to the small volumes. The mixing process is greatly simplified by use of a stock solution consisting of United States Pharmocopeia (USP) 88% phenol 24 ml and croton oil 1 ml. This solution yields a concentration of 0.04 ml croton oil/1 ml stock solution. By increasing the volume of the ingredients they are easily measured with accuracy using standard syringes. By varying the relative volumes of phenol acid and stock solution, different croton oil concentrations are possible using standard tables ( Table 2.1 ).
| Croton oil | 0.2% | 0.4% | 0.8% | 1.2% | 1.6% |
| Water | 5.5 ml | 5.5 ml | 5.5 ml | 5.5 ml | 5.5 ml |
| Septisol | 0.5 ml | 0.5 ml | 0.5 ml | 0.5 ml | 0.5 ml |
| USP phenol 88% | 3.5 ml | 3.0 ml | 2.0 ml | 1.0 ml | 0.0 ml |
| Stock solution containing phenol and croton oil | 0.5 ml | 1.0 ml | 2.0 ml | 3.0 ml | 4.0 ml |
| Total | 10 ml | 10 ml | 10 ml | 10 ml | 10 ml |
| 0.1% = 1 ml of 0.4% + 1.2 ml phenol + 1.8 ml water | |||||
| 0.05% = 1 ml of 0.2% + 1.2 ml phenol + 1.8 ml water | |||||
| Stock solution = 24 ml phenol + 1 ml croton oil | |||||
| (0.04 ml croton oil) or 4% croton oil | |||||
| (1 ml stock solution) | |||||
As an example, to make a 0.4% croton oil solution, one would mix water 5.5 ml, Septisol 0.5 ml, and add USP phenol 88% 3 ml and stock solution 1 ml. This 1 ml of stock solution contains croton oil 0.04 ml. Because the total volume is 10 ml, the final concentration is 0.04 ml of croton oil in 10 ml total volume or 0.4%. To make weaker concentrations such as 0.1% and 0.05%, one first makes 0.4% and 0.2% and these are further diluted as shown on the table. The final concentration of phenol with all these formulas is 35% by volume. The stock solution at 4% croton oil is always meant to be diluted and should never be applied to the skin full strength.
A more recent variation is to add olive oil at a final concentration of 15% by volume. The addition of olive oil has a tempering effect on the absorption and allows more even distribution of the solution. In the 10 ml solutions, the water volume would be 4.0 ml and olive oil 1.5 ml. In the weaker croton oil solution such as 0.1% where the total volume is 4 ml, the water volume would be 1.2 ml and the olive oil volume would be 0.6 ml. Another useful variation is to prepare a solution with a higher concentration phenol, such as 60% with a weak concentration of croton oil, such as 0.1% or 0.05% to use in instances where pigmentation is more of an issue rather than wrinkles. In the 4 ml solutions, the water volume would be 0.95 ml and the phenol volume 2.05 ml.
Intra-operative routine
Usually the peel is performed with intravenous sedation or general anesthesia. It is important to provide a pain-free emergence from anesthesia and a comfortable post-peel course. If this is done, the entire recovery and general experience will be much better. Standard facial nerve blocks (supra-orbital, infra-orbital, supra-trochlear, zygomatico-facial, zygomatico-temporal, mental, and Erb’s point) are performed with bupivicaine with epinephrine as well as subcutaneous infiltration of dilute (0.125%) plain bupivacaine throughout the operative site. These are important steps as the peel is quite stimulating. Intramuscular ketorolac tromethamine can be given as an adjunct unless an operative procedure is being performed at the same time. Intraoperative steroids are administered and are followed by a Medrol Dosepak the next day.
Ophthalmic ointment and corneal protectors are not used because phenol may dissolve in the ointment preventing immediate flushing out if it becomes necessary. Extreme care must be taken around the eyes at all times. The skin is degreased with acetone and patients are told not to apply anything on the skin on the day of the peel. Historically, fear of cardiac complications has been associated with phenol peels, but reports of death are anecdotal, and it is difficult to blame phenol toxicity as the cause. Although arrhythmias in the course of peeling are well documented, they are uncommon and rarely require treatment. There is speculation that arrythmias may be caused by the intense stimulation brought about by a high concentration of croton oil. With the lower concentrations of croton oil in the modern peels, lower concentrations of phenol (35% vs 49%), and careful attention to local anesthesia of the face, cardiac complications have not been a problem. Standard precautions include cardiac monitoring, adequate hydration, and performing a full face peel in no less than 45 min.
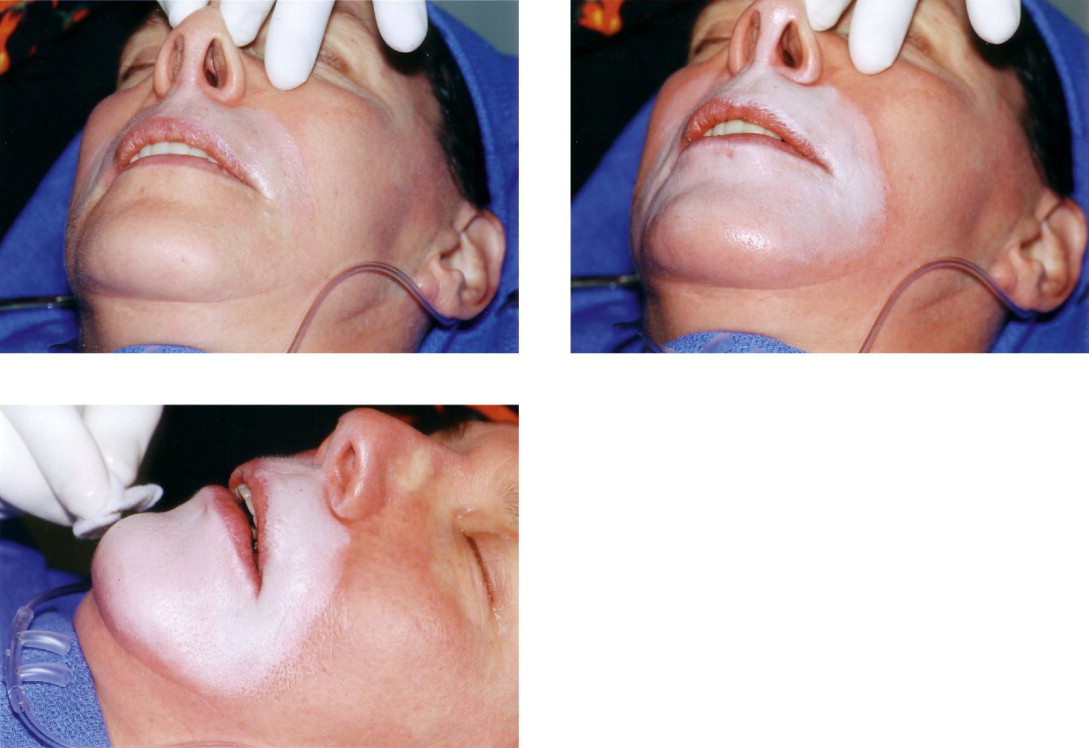
Application
The different concentrations are placed in separate, easily identifiable bowls or cups. The applying materials are 2 × 2 gauze and cotton-tipped applicators. This gauze is dipped into the solution and carefully wrung out. The mixture is stirred prior to each application. An assistant helps dry the applying hand in order to prevent inadvertent application where it is not wanted. One must exercise constant vigilance in this respect. With the damp gauze in hand, multiple rubbings are made, observing the color change of the skin. The effect of the peel is to create a ‘frost’. The acid coagulates and precipitates the protein, forming a frost, which is a way of describing varying degrees of a white appearance. As the application progresses, the depth is gauged by the degree of frosting which becomes progressively more dense ( Figures 2.1–2.3 ). The speed of the appearance of the frost depends on the concentration used and how wet the gauze is. With the typical concentrations described and using a damp gauze, the appearance of the frost is gradual and can be seen in 10–20 seconds. Unlike peels with trichloroacetic acid (TCA), there is no need to wait several minutes to see the final depth.