Edwin Cortez, Fred Fedok, and Devinder Mangat address questions for discussion and debate. Do you agree or disagree, and why, with the following: “The best method to improve moderate to deep rhytids is the croton oil–phenol peel.” “There are no problems with cardiotoxicity with croton oil–phenol peels if done appropriately.” “Do not do spot testing with chemical peel agents.” How do you handle peels in advanced Fitzpatrick skin types III, IV, V? What is the main factor for rate of reepithelialization: (1) depth of peel, (2) depth of laser, (3) depth of dermabrasion? How has your approach to or technique in chemical peels evolved over the past several years?
Edwin Cortez, Fred Fedok, and Devinder Mangat address questions for discussion and debate:
- 1.
- 2.
- 3.
- 4.
How do you handle peels in advanced Fitzpatrick skin types III, IV, V?
- 5.
- 6.
Do you agree or disagree, and why, with the following: “the best method to improve moderate to deep rhytids is the croton oil–phenol peel.”
Cortez
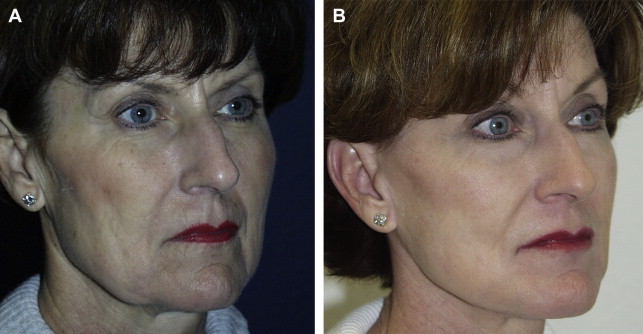
I fully agree with the statement that “the best method to improve moderate to deep rhytids is the croton oil–phenol peel ( [CR] ).” Phenol–croton oil peeling is still the standard against which all other treatment regimens for photodamaged skin are measured. In my practice, this modality is still the most safe, cost-efficient, and long-term treatment for treating medium and coarse facial rhytids. Figs. 1 and 2 show 2 of our patients before and after treatment.

The long-term criticisms of the standard Baker-Gordon peel are no longer valid. Since the elegant studies by Hetter and Stone, the entire spectrum of croton oil–phenol peeling has finally become scientifically validated. For many years, we were very pleased with our results from the Baker-Gordon formula but we have now created our own modification, which will be discussed in response to a different discussion. We have observed patients for over 25 years after being treated with croton oil–phenol preparations, and the long-term results are excellent. We are now seeing patients who we treated in their 50s and are now in their 70s and still have beautiful, firm, non-photodamaged skin. I have used dermabrasion for rhytids in the past, but in this day of problems with infectious diseases, including human immunodeficiency virus, hepatitis C, and so forth, I would prefer not to have aerosolization in my operating suite.
In the early 1990s we saw a dramatic shift to laser ablative resurfacing with the CO 2 laser. This modality was supposed to be free of any serious postoperative sequelae, such as hypopigmentation. However, 2 years after large numbers of cases were performed with the CO 2 laser, many patients were seen who developed severe hypopigmentation and also scarring and texture changes, and so forth. Now, many have put their CO 2 lasers in the garage and a new era of fractional CO 2 laser resurfacing has been born. We all hope that this expensive laser lives up to industries’ promises!
In summary, to date, we still find the croton oil–phenol peel as the best and safest modality for the treatment of moderate and deep rhytids.
Fedok
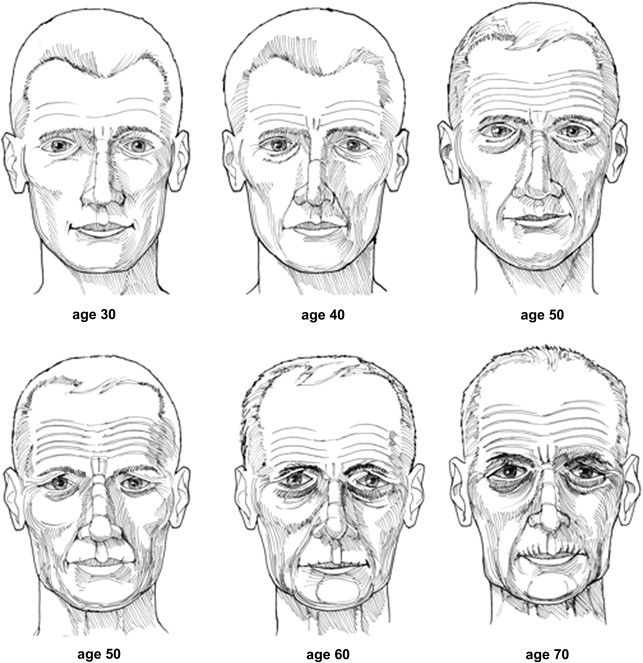
The term “rhytids” describes the wrinkled appearance of the skin caused by the decrease in skin elasticity, decrease in skin water content, and changes in collagen crosslinking that typically occurs with aging. In patients with milder aging effects, the rhytids are fairly superficial and the derangement of the anatomy is isolated to more superficial aspects of the epidermis and dermis, such as might be present in the facial skin of patients in their third decade. With more advanced skin aging the involutional and photoaging changes are more pronounced and involve deeper aspects of the dermis. In the former situation, such as in the younger patient, the rhytids usually make their early appearance around the “crow-feet” area and are largely noticeable with movement, such as smiling. In the latter situation more typical of the older patient, the rhytids may be present at repose and actually produce folds of lax skin with movement ( Fig. 3 ).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


