Cheek Reconstruction With Laterally or Medially Based Cervicofacial Flap
Sammy Sinno
Barry M. Zide
DEFINITION
Local tissue from the cheek and upper neck provide the best tissue for cheek reconstruction; several techniques have been described including submental and sternocleidomastoid flaps.1,2
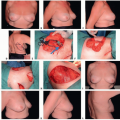
Laterally, or posteriorly, based cervicofacial flaps are most useful for small to moderate full-thickness skin and subcutaneous defects of the anterior and inferior cheek. These flaps take advantage of the loose neck skin to provide a large amount of coverage with local/regional tissue borrowed from the lateral face, neck, and even chest. Laterally based flaps avoid incisions below the eyelid; however, crossing the anterior mandibular border may require a Z-plasty (FIG 1).
Medially, or anteriorly, based cervicofacial flaps are also useful for moderate sized full-thickness skin and subcutaneous defects of the anterior and upper cheek. These flaps also take advantage of the loose preauricular and neck skin and avoid incisions on the mandible.
 FIG 1 • Lateral-based and medial-based cheek flaps. |
ANATOMY
The cheek is a laminated structure consisting of skin, subcutaneous tissue, and the superficial musculoaponeurotic system (SMAS). These structures overlie the facial nerve, parotid gland, buccal fat bad, and mandible.
The arterial supply to the cheek is provided by the facial, superficial temporal, and transverse facial arteries originating from the external carotid artery. Venous drainage may parallel the arterial system though variations are common (FIG 2).
Techniques of deep-plane elevation or tissue expansion can be used to improve the blood supply and reliability of the flap.2,3,4,5
The cheek can be subdivided into overlapping zones to categorize lesions and organize the reconstructive strategy (FIG 3).
PATIENT HISTORY AND PHYSICAL FINDINGS
The cheeks are often exposed to trauma and sun damage leading to a frequent requirement for reconstruction.
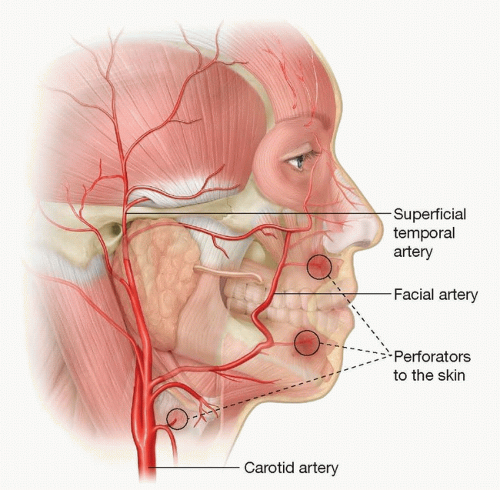
FIG 2 • Arterial blood supply of the cheek.
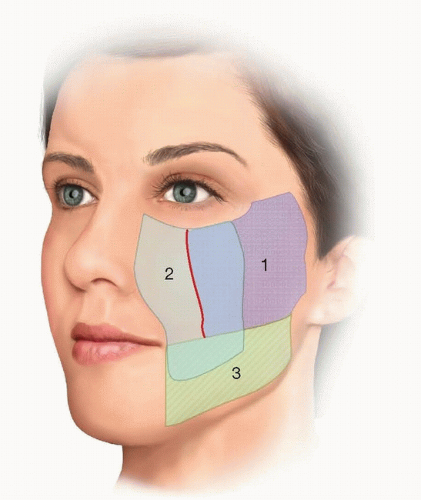
FIG 3 • The three reconstructive zones of the cheek. Red border between zones 1 and 2 marks a vertical line dropped from the midpupil. Zone 1, lateral cheek; zone 2, central cheek; zone 3, inferomedial cheek. Laterally (posteriorly) based cheek flaps work best for zone 3 defects. Medially (anteriorly) based flaps are best for zone 1 and 2 defects.
The defect size, depth, and location must be evaluated in addition to the surrounding skin quality, tone, and texture.
Hairlines should also be noted, particularly sideburns in women, as this will affect flap design due to the need to avoid hair transposition onto the cheek.
Patients should be encouraged to stop smoking as this increases the risk of distal flap necrosis.
For skin cancer defects, consider delaying the reconstruction until the resection margins are proven clear by histological analysis.
The effect of radiation therapy must also be taken into account when applicable.
Ensure that the blood supply to the face is intact by evaluating neck and facial scars.
Specifically evaluate the area where the facial and superficial temporal arteries are located. Pay particular attention to prior sentinel lymph node biopsy scars in the face and cheek.
IMAGING
No imaging is required other than that indicated by a preoperative clearance workup.
SURGICAL MANAGEMENT
Preoperative Planning
Smaller cervicofacial flaps may be performed under local anesthesia or deeper anesthetic techniques.
Assess the mobility and laxity of the skin surrounding the defect and determine which facial structures may be distorted by flap movement.
Scars should be positioned at the border of aesthetic units (nasal-facial junction, nasolabial fold, infraorbital rim) or along the hairline when possible, which may require sacrifice of additional tissue.
If it is not possible to place the scar at the border of aesthetic units, scars should be aligned parallel to relaxed skin tension lines (these are curvilinear on the cheek).
Positioning
Patient is positioned supine on the operative table with the head turned to the contralateral side from the defect.
The ipsilateral face, neck, and chest are prepped into the field. Alternatively, the entire face may be prepped into the field to assess symmetry intraoperatively.
Approach
Depending on the size and location of the defect, decisions must be made regarding plane of flap elevation (subcutaneous or sub-SMAS), extent of posterior incision (preauricular, postauricular, chest), and need for preoperative tissue expansion.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree