Cheek Reconstruction With Free Radial Forearm Flap
John G. Fernandez
DEFINITION
Cheek and face defects commonly occur secondary to trauma, burns, or tumor resection.
Most cheek defects can be treated with primary closure, skin grafts, or local flaps.1
Less commonly, reconstruction of cheek defects requires free flap transfer. These defects are more complex, often involve a large area of the skin, or are composite defects involving the cheek skin and underlying tissues.
Free flap coverage is necessary owing to lack of local tissues from previous surgery or radiation.2
Some patients require free tissue transfer because the facial vessels are ligated during the course of concomitant neck dissection.
The radial forearm flap (RFF) is an excellent option in these situations due to its long pedicle, thin and pliable skin paddle, and the potential to transfer multiple skin paddles to line composite through-and-through cheek defects.
Other flaps are also useful for cheek defects. These include the anterolateral thigh flap, scapular and parascapular flaps, lateral arm flap, fibula flap, and the rectus abdominis flap.
Flap selection is based on multiple factors including volume of tissue loss and subsequent functional and aesthetic reconstruction needs.
This process is individualized for the patient and the defect to be reconstructed.
No clear evidence supports one flap over the use of another.
The flap must appropriately match the color and thickness of the surrounding cheek soft tissue and have a reliable blood supply with adequate vessel diameter and length.
The advantage of RFF is its flexibility in design and its ability to be fashioned as a fasciocutaneous flap, as an osteocutaneous flap involving unicortical short segment of radius, or as composite flaps, including palmaris longus tendon (for lip reconstruction), as well as its ability to be de-epithelialized and folded to reconstruct the intraoral lining and external skin defects.2
ANATOMY
The borders of the cheek include laterally the preauricular crease, medially the nasal-cheek junction, nasolabial fold and lip, inferiorly the lower border of the mandible, and superiorly the orbital-cheek junction (FIG 1A).1
The main arterial supply to the cheek is from branches of the external carotid artery with the greatest contribution arising from the facial artery.
The branches of the facial nerve lie deep to the SMAS.
The RFF venous drainage is primarily from the venae comitantes, secondary drainage from the cephalic vein (FIG 1B).3
RFF dominant arterial supply is the radial artery.
PATIENT HISTORY AND PHYSICAL FINDINGS
The history should identify patient factors that may increase the risk of complications, including smoking history, hypertension, obesity, diabetes, and prior radiation therapy.
Elicit personal or family history of clotting abnormalities, strokes, coronary artery disease, or cerebrovascular disease.
A personal or family history of clotting abnormalities may warrant a hematology consult to rule out familial causes of hypercoagulability or bleeding diathesis.
A directed physical examination of the head and neck includes a detailed assessment of the tumor or traumatic defect; nodal involvement; quality of the surrounding cheek skin including laxity, scars, and fine wrinkles; and assessment of facial nerve function.
Preoperative plan for resection should be determined in consultation with the oncologic surgeons.
Orbital-cheek junction and periorbital reconstruction may result in eye-related complications including ectropion, scleral show, dry eye, and chemosis.4 Therefore, a preoperative and postoperative visual field exam and periorbital assessment may be necessary for lesions that encroach on the eyelid.
The preoperative evaluation for patients who will undergo cheek reconstruction with an RFF flap includes gathering pertinent patient history such as hand dominance, prior upper extremity surgery, history of trauma, or fractures.
Consider the body habitus and thickness of the donor tissue and its potential effect on the overall aesthetic and functional outcome.
An Allen test should be performed to assess ulnar and radial artery perfusion to the hand. Motor and sensory examination of the hand should be performed.
Patients should be instructed to avoid blood draws or intravenous line placement in the arm to be used for RFF harvest.
IMAGING
X-ray of the forearm and hand is indicated if an osteocutaneous flap is planned.
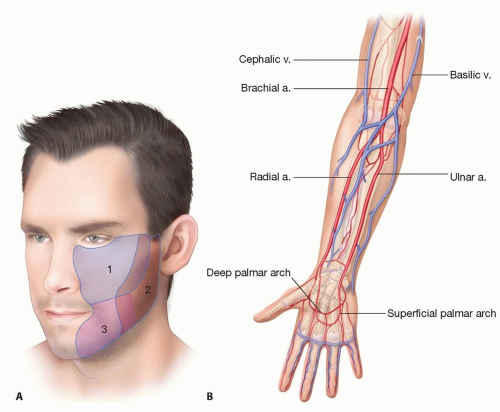 FIG 1 • A. Outlines of the zones of the cheek. Note overlap of zones. B. Arterial and venous anatomy of the forearm. |
SURGICAL MANAGEMENT
The goal of surgical management is to re-establish the normal anatomy of the face; provide stable soft tissue coverage; allow for normal speech and swallowing, thereby improving quality of life; and maximize aesthetics.
An RFF is an excellent option for complex defects of the cheek and can be performed to provide external coverage or as a folded flap to repair through-and-through cheek defects.
Preoperative Planning
Consider the size of the anticipated defect of the aesthetic subunit (suborbital, preauricular, and buccomandibular) and intraoral component (if any).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree