Summary
There are three anatomic zones, the suborbital, preauricular, and buccomandibular (zones 1, 2 and 3, respectively), to consider when reconstructing the cheek.
Direct closure, even for large defects, often provides the most ideal result.
Cervicofacial advancement flaps can be performed under intravenous sedation with very low complication rate. 1
Lower eyelid complications can be avoided by appropriate flap design that includes the cheek–lid junction incision and lateral placement of vertical flap tension vector.
Full-thickness grafting can be preferable for medial cheek defects but should be used with caution for larger central defects.
16.1 Algorithm for Closure (▶ Fig. 16.1 and ▶ Fig. 16.2)
16.1.1 General Considerations
In evaluating the cheek, there are important functional considerations and it is useful to consider the anatomic zones defined as follows: zone 1—the suborbital and premolar medial cheek from eyelid to below malar eminence; zone 2—the temporal/preauricular; and zone 3—the buccomandibular from below malar eminence to mandibular rim (▶ Fig. 16.1 and ▶ Fig. 16.2). 2 The primary factor of zone 1 is the functional integrity of the lower lid and a successful cheek reconstruction is a failure if there is extrinsic ectropion, which is the most common complication of these procedures and is entirely avoidable with appropriate techniques. Also, zone 1 contains the malar eminence, or the malar prominence, and this is often quite a difficult area to reconstruct due to convexity with limited tissue laxity from anterior to posterior plane. Additionally, it is the most prominent anatomic location on the cheek.
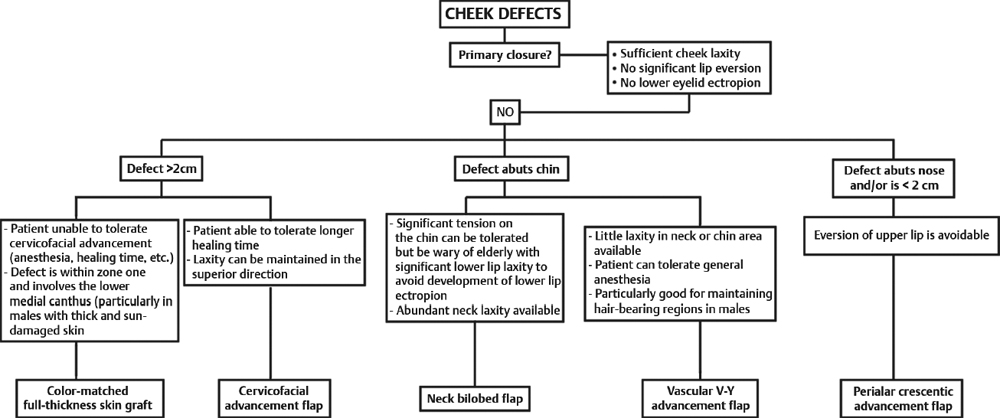
Fig. 16.1 Algorithm for cheek closure.
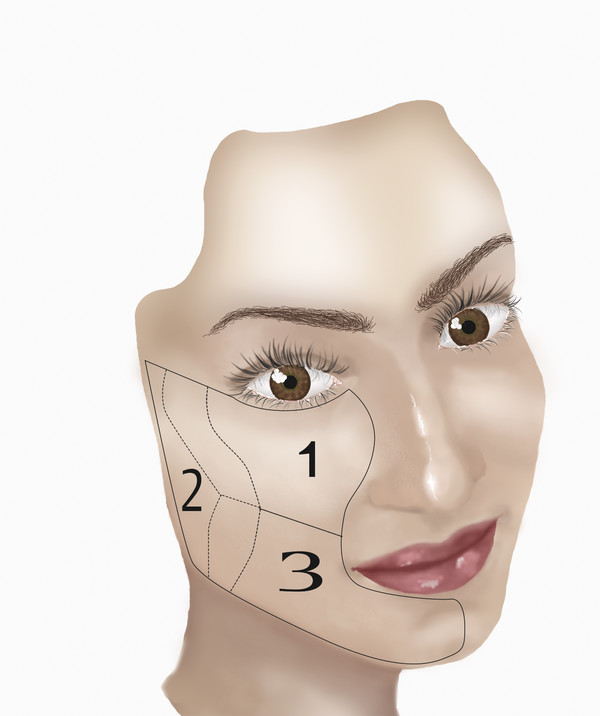
Fig. 16.2 The three anatomic zones of the cheek: zone 1, suborbital and premolar; zone 2, the temporal/preauricular; and zone 3, the central cheek to mandibular rim.
Zone 2 is reasonably featureless. It is limited posteriorly by the ear and therefore there is functional significance to maintain the patency and configuration of the external auditory canal. What is most challenging on zone 2 is that it is a zone of adhesion and, despite being relatively flat and featureless, has relatively little laxity in the anteroposterior plane and this must be a consideration for reconstructive planning. 2, 3 Importantly, zone 2 is somewhat posterior and hidden from frontal viewing and more liberty can be taken with incision placement and secondary healing.
Zone 3 has functional importance with regard to the lower lip, and it must remain in its anatomical position to maintain oral competence. Additionally, zone 3 includes the convexity of the chin and it has little inherent laxity to recruit for reconstruction.
16.1.2 Commonly Applied Methods of Closure
Primary closure utilizing the laxity of the cheek and oriented in the vertical plane to reduce risk of lower eyelid ectropion.
Combined chin and cheek defects (zone 3) may tolerate primary closure with avoidance of lower vermilion ectropion; however, in the elderly patients with significant lower face laxity, a bilobed flap advanced from the neck may be a preferable postoperative result.
V-Y advancement flap is often an excellent choice for either lateral or medial chin defects as well as defects found on the upper cutaneous lip. These may be especially useful for small defects in males restoring hair bearing coverage.
Defects of the upper cutaneous lip may ideally be managed with a perialar crescentic advancement flap; care must be taken to avoid eversion of the upper lip.
For patients that may not tolerate a cervicofacial advancement flap, color-matched full-thickness skin grafting is a safe and viable option.
16.2 Primary Closure
The algorithm for cheek reconstruction begins with attempts at primary closure. A single tacking suture is placed sequentially in two orientations at 180 degrees from each other and the wound is tailor tack closed. Even large linear scars on the cheek heal tremendously well and this is considered a first choice reconstruction. 2 Linear closures on the midportion in zones 1 and 2 of the cheek are vertically oriented to prevent ectropion. The resulting dog-ear or standing cone can be extended into the cheek–lid junction. This often involves the lower eyelid and as long as meticulous attention is paid to elimination of redundant skin on the final inset, excellent results can be obtained. Rarely any attempt is made at undermining given there is more than sufficient laxity for the vast majority of defects to affect a mild tension closure. Vigorous postoperative scar management, including early use of silicone sheeting, adjunctive laser treatment, and dermabrasion as required are critical to obtain ideal postoperative results. 4, 5, 6 The clinical examples illustrated show both short- and long-term results for linear closures. These were female patients without ideal skin tone or type for optimal linear closure; however, with closure even under moderate tension, the final results with minimal postoperative adjunctive methods are superior to any other technique. The consideration or institutional avoidance of transposition flaps for the cheek is based on the fact that even the most properly done transposition flap will, by definition, have surgical incisions placed counter to ideal relaxed skin tension lines. The very premise of a transposition flap is to recruit laxity from an area of relative laxity to an area of a paucity of laxity and on the cheek we consider the entire anatomical subunit to have essentially equal laxity. 7 Therefore, there is simply no surgical advantage of transposition flaps on the cheek and additionally they lead to suboptimal scarring patterns. Clinical example 3 shows the poor postoperative result from an adequately designed and executed rhomboid transposition flap for cheek reconstruction (▶ Fig. 16.3, ▶ Fig. 16.4, ▶ Fig. 16.5).

Fig. 16.3 A 62-year-old female with an appropriately designed and executed rhomboid flap for cheek closure. This illustrates the postoperative deformity inherent in geometric flap closure of cheek defects.

Fig. 16.4 A 48-year-old female status post 2 × 3 cm Mohs excision for basal cell carcinoma at right malar cheek. Defect was closed primarily with standing cone excision. Postoperative results shown at 1 and 3 months from left to right. Note that lip eversion seen immediately postoperatively settled by 3 weeks.

Fig. 16.5 A 54-year-old female status post 1 × 1 cm Mohs excision for basal cell carcinoma on the left malar cheek. Wound was treated with primary vertical closure and standing cone excision. Postoperative results shown at 1 week, 1 month, and 6 months, from left to right.
16.3 V-Y Advancement Flap
A V-Y advancement flap has been defined for both central and lateral cheek defects and is effective for very large and complete defects. Several technical points on this is that once a single perforator vessel is identified with Doppler, generous soft-tissue advancement can be performed if this single vessel is maintained. 8 Very wide dissection is then possible. When these have been performed and appropriately inset, the final results on these flaps are quite good, with provision for re-advancement if needed (▶ Fig. 16.6).

Fig. 16.6 A 68-year-old white male status post 4 × 3 cm Mohs excision for melanoma in situ on right nasomalar region. Wound was closed with a V-Y advancement flap and full-thickness skin graft at the alar base. Postoperative results shown intraoperatively at 1 and 10 months, from left to right.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


