CHAPTER 9 The Male Neck
Summary
This chapter describes how to address the aging neck in isolation. Like any other aspect of medicine, correct treatment cannot be executed without the correct diagnosis. First the readers are taken through the appropriate physical examination features to note to establish the most efficient surgical plan. Then, step-by-step, each surgical maneuver is described with appropriate anatomical correlation, so that the readers can execute the surgery in their own operating rooms. We also review major decision tree steps such as when to open the neck or treat it with closed liposuction. We then discuss complications and how to manage them. Finally, postoperative care details are reviewed to ensure that any differences that can be made in aftercare acknowledged and described.
Introduction
Neck rejuvenation in men is more commonly sought as an isolated procedure than it is in women. Men tend to look the same, regardless of their haircut or clothing. This is different from women who routinely change their appearance with either a new hairstyle or can contrast their appearance from casual to formal with the assistance of their clothing choices. For this reason, men commonly avoid any procedure that will dramatically change the way they appear, even if for the better. The two most common facial areas men seek improvement for are their eyes and their neck.
Historically speaking, neck lifts are accompanied by face-lifts. This makes sense because the two regions anatomically overlap. Most significant tightening of the neck will yield at least some “dog ear” on the face that must be dealt with, and vice versa; any significant tightening of the lower third of the face will yield excess neck skin that also must be excised and redraped (usually behind the ear).
Nonetheless, men frequently desire improvement in the neck without change to the face. In our practice, this is usually accomplished with one of three modalities:
Isolated male neck lift.
Direct neck lift with or without Z-plasty (usually without).
Neck liposuction, with or without placement of a chin implant.
This chapter focuses on the isolated neck lift with platysmaplasty.
Physical Evaluation
Evaluate for the presence of neck skin laxity. This should be present in all men seeking an isolated neck lift. If not, it is possible their complaint is more related to their jowls, and a traditional face-lift would be more appropriate.
Determine the presence of platysma bands. There are active and passive bands. Active bands can be seen during elocution. Passive bands are hard to distinguish from excess skin and are usually adhered to the excess skin. These can be identified by having the patients show their bottom teeth and fire their lower lip depressors (say “eeee”).
Because an isolated neck lift requires retroauricular incisions with extension into the hairline, the hairline should be evaluated as a suitable region to place a scar. The closer the hairline begins to the ear, the easier it is to hide the incision. For men with thin hair or no hair, a decision must be made whether to compromise the vector of the pull by not extending the incision out of the retroauricular sulcus or to accept a potentially visible, though usually well-healed scar.
Presence of facial hair should be noted. Usually, patients are asked to grow a short beard prior to surgery to help conceal evidence of surgery.
Note should also be taken of the preauricular region—specifically location of the beard hairline in relation to the ear as well as the skin quality, texture, and pore size of the preauricular region. This is to help determine the suitability of a patient for either a preauricular or intratragal incision.
Anatomy
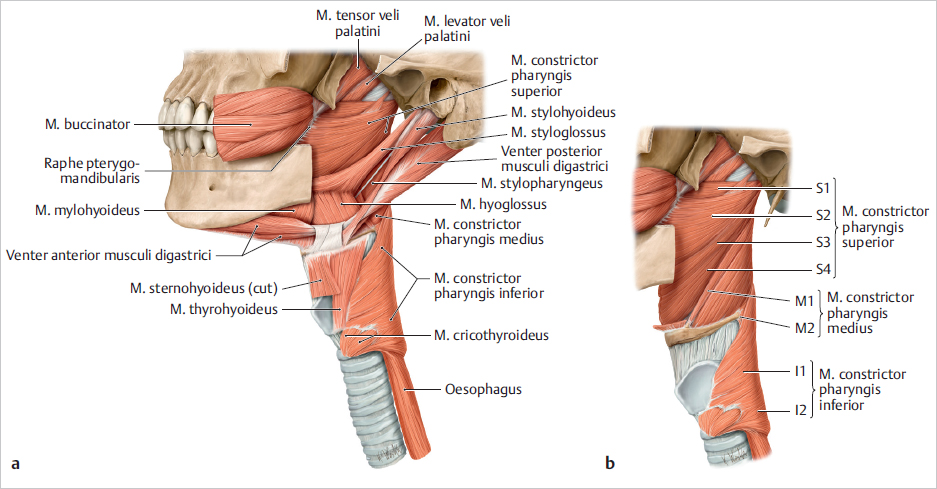
Anatomical considerations for this procedure are best divided by region according to the steps of the procedure ( Fig. 9.1 ). First, the submentum is addressed. There are no structures of significant concern in the subcutaneous region of the direct submentum. There are, however, bridging veins that can be adherent to the dermis of the skin. Especially in older patients with thin skin, these can become troublesome and are best dealt with by avoiding them altogether. This is accomplished by endeavoring to leave a layer of fat on the submental skin flap. If a vein is encountered, insulated forceps and a very low setting on the electrocautery can maintain control. Alternatively, the area can be packed and then ultimately compressed with a tight dressing.
The area of concern in the neck exists beneath the platysma, where the marginal mandibular branch of the facial nerve lives as well as larger vessels like the anterior jugular and branches of them that can be inadvertently entered.
Further, the surgeon should discuss the presence of submandibular glands prior to neck surgery. Often, these are prominent and contribute to an imperfect neck contour. The authors do not offer removal of the submandibular glands. We explain these glands produce approximately 50% of their saliva and removal could result in dry mouth—especially with age. Further, there are inherent dangers to removing the gland—but certainly ones that can be overcome.
Steps for Isolated Neck Lift with Platysmaplasty
Defatting the Neck and Jowls
Whenever possible, we prefer closed suctionassisted lipoplasty in the neck and jowls. We use a 2.4-mm Mercedes tip cannula, keeping it under constant, steady motion in the subcutaneous space. The goal is to leave a layer of subcutaneous fat on the undersurface of the cervical skin. If we suction the jowls, this is always done conservatively.
We rarely suction or remove subplatysmal fat, because (1) the facial nerves run just beneath the platysma, and (2) any patient with significant subplatysmal fat probably has a fat, round face, so removing subplatysmal fat could create an overoperated look.
Usually, we perform lipoplasty before elevating the skin flaps. However, it is reasonable to perform this lipoplasty after redraping of the skin flaps, so that the portion of the superficial muscular aponeurotic system (SMAS)-platysma that will be elevated over the mandible is not oversuctioned.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


