Chapter 52 COMPLICATIONS
Although fat grafting procedures have an established record of safety, and reports of adverse outcomes are infrequent, complications do occur, as with any surgical procedure. Most complications are related to aesthetic appearance and are most often associated with the location, manner, and volume in which the fatty tissue is placed into recipient areas. These include overcorrection, undercorrection, visible irregularities, migration of injected fat, and donor site problems. 1 Improvement in a patient’s facial or body contours is not always enough to produce a satisfactory result. One of the most difficult elements of fat grafting is reliably determining what the patient desires before the procedure and what result will make the patient happy; often these are not the same. 2 If the patient is not psychologically prepared for changes in the face or body and is not thoroughly educated about the postprocedure course and the potential for unexpected events, an otherwise successful procedure can yield disappointing results. The surgeon must be familiar with the complications associated with fat grafting and should warn the patient about the problems that are most likely to occur during a fat grafting procedure. Before the operation starts, the patient should carefully read and understand the informed consent form, in which all the details of the planned procedure are accurately explained, as well as the predicted outcome, the postoperative course, the patient’s responsibilities during recovery, and potential sequelae and complications.
Structural fat grafting has other potential complications; for example, infection; damage to underlying structures such as nerves, muscles, and glands; necrosis; calcifications; the formation of oil cysts; and most critically, embolism.
Fortunately, the complication rate with fat grafting is extremely low compared with most open surgical techniques, and the incidence of unpleasant events decreases significantly with surgeon experience.
Common Aesthetic Complications
INSUFFICIENT VOLUME
The goal of structural fat grafting is to have the grafted fat survive evenly and predictably. The most common complaint that patients have after the swelling subsides is that they had expected more or less fullness in a specific area. There are numerous factors to consider when estimating the volumes of fat to be grafted, including the resorption rate and the intraoperative occurrence of edema. Obtaining the exact amount of fullness that will satisfy a patient can be difficult. Careful planning and fat preparation are essential (see Chapter 1). Even after the physician and patient agree on the desired change, many variables will affect the outcome (see Chapter 2). Surgeons are frequently asked how much of the grafted fat will survive. At present, it is not possible to give an exact answer. A good approach is to look at the photographs of the patient when he or she returns for follow-up, observing the volume of fat that was grafted to produce a specific change. It is important to understand what different amounts will do rather than focusing on the question of how much will survive. Thus it is even more important to know what 10 cc of fat placed in the face will look like compared with 20 or 30 cc.
RESORPTION
When edema subsides and the patient expected more fullness, the question is whether this adverse outcome is related to insufficient placement or to resorption. Resorption represents one of the main drawbacks of the procedure; it has been reported to range from 25% to 80%. 3 , 4 Fortunately, numerous means are available to reduce the resorption rate as much as possible.
Obtaining Pure Fat
Ideally, one should obtain the purest fat possible by eliminating the blood and oily components of the lipoaspirate along with other debris, while handling the material in such a way to incur minimal damage to the adipose tissue (see Chapter 1). The presence of blood, fatty acids, and other debris seems to stimulate an inflammatory response, which induces resorption. No matter how carefully the fat is prepared, it will not be 100% “pure.” Varying degrees of oil, blood, and other impurities, such as lidocaine, will be present in the lipoaspirate, even after processing. Furthermore, a varying degree of the refined material placed will not be viable. Despite meticulous technique, a portion of the fatty tissue will die from the negative pressure, exposure to air, and mechanical trauma sustained during harvesting and refinement of the fragile fatty tissue.
Reducing Trauma
Forcing the lipoaspirate through a small cannula places a positive pressure and further mechanical trauma on the fatty tissue parcels. This trauma can vary from patient to patient. For instance, in thin patients, the fat cells store much less triglyceride, which makes the cells smaller. When the tissue parcels are composed of smaller cells, they are more likely to flow through the cannulas without rupturing. In heavier patients, the fat cells are engorged with triglycerides and are therefore larger. These larger cells, with stretched cell walls, can be more easily ruptured by the mechanical maneuvers associated with harvesting, purification, and placement. It is difficult to predict the exact percentage of tissue that will be lost in these steps.
Preserving Viability
Because the transplanted fat is often located at an inconsistent distance from a blood supply, some of the injected fat will die in an irregular fashion. As the tissue necroses and resorbs, irregularities occur. This may happen as late as 4 or more months after the procedure, when swelling subsides. Placement of a lump of tissue, rather than a small aliquot, with the intent to mold it into a specific shape will frequently result in irregularities.
Even under ideal circumstances, a small portion of transplanted fat will die, but certain conditions increase the likelihood of fat necrosis. Ischemia represents the major cause.
Placing Minimal Aliquots of Fat
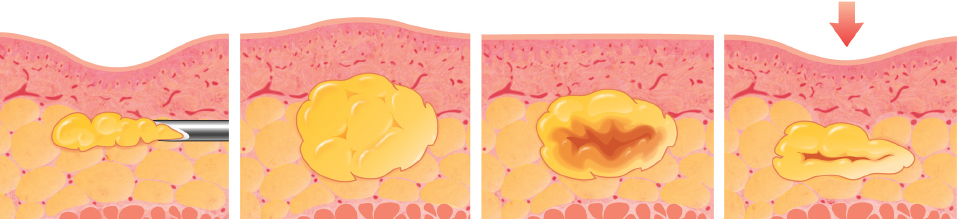
Placement of an excessive amount of fat as a bolus isolates the transplanted cells in the center of the lump from a blood supply. Without nutrition and respiration, these cells may die. The result is likely the formation of oil cysts, calcifications, and fibrosis. 4
It is essential to avoid injecting a bolus, which will induce necrosis of the central portion of the transplanted adipocytes. Placement of minimal aliquots of fat maximizes the contact and favors the successful take of the graft. Forcing too much tissue into a limited recipient site such as the nose, or placing the grafted fat in too thick a layer (such as filling a deep sternal defect) can result in necrosis, because the grafted tissue does not receive adequate nutrition or respiration. Over the long term, tissue atrophy, oil cyst formation, and progressive calcification develop.
SWELLING
Postprocedure edema is the most common problem associated with structural fat grafting. Patients need to be well prepared for their postoperative appearance so that they are not unduly alarmed by the degree of swelling that occurs. It is also important to warn patients that this adverse situation will continue to increase for up to 3 days after the procedure so that they do not panic when they notice this. The injection of a local anesthetic into the tissues can swell and “pump” the tissues full of solution. The amount of local anesthetic should be minimized to the smallest volume that will numb the area and obtain vasoconstriction with a minimum of distortion. Electrotherapy devices have been used successfully for 5 to 7 days in rhytidectomy, liposculpture, and facial fat grafting to reduce swelling following surgery. 5
How Edema Occurs
Forcing a blunt cannula through living tissue will immediately provoke edema. In injecting separate tiny parcels of fat, hundreds of passes may be made with a blunt cannula; the end result is an alarming amount of edema.
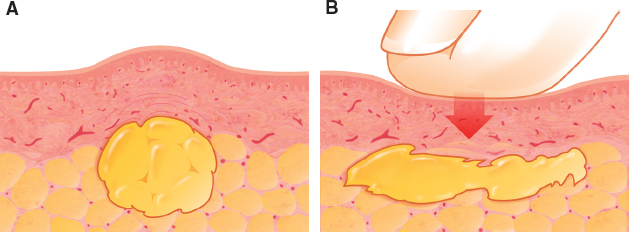
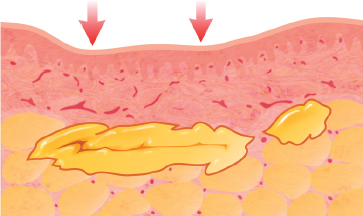
Many early authorities on fat grafting have advocated molding of the fatty tissue after placement to create the desired shape, to distribute the fatty tissue evenly, and to smooth out any surface irregularities. After placement of as much as 1 or 2 cc of fat at each pass, these surgeons recommend using digital pressure to redistribute the fatty tissues. Unfortunately, this type of maneuver affords little control over the subdermal configuration of the manipulated volume, and the fat may even squirt in many directions to form irregular pools of tissue.
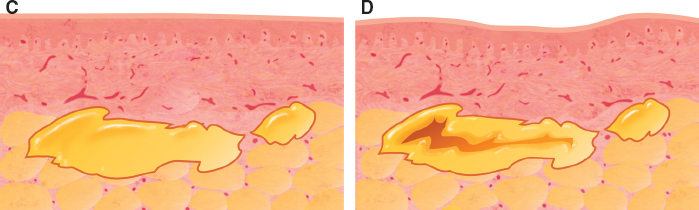
As previously noted, unequal access to nutrition and respiration can cause irregular survival of the fat, which results in surface irregularities. If a cyst or clump forms accidentally, digital manipulation can sometimes flatten such minor irregularities. However, the tissue should never be placed with the idea that digital pressure can change the shape after placement. The edema that is created by fat placement and subsequent manipulation can confuse a novice surgeon into believing that because the swollen skin surface initially appears smooth, the underlying graft has been adequately placed in a smooth layer. If the fat were all to survive, the surface would remain smooth; however, a portion of fat often dies.
This obscures the visual clues that might be helpful for determining an endpoint. Also, because of individual patient variations, it can be difficult to predict how a given patient’s body will react during and immediately after the injection of fatty tissue.
This three-dimensional technique of placing refined fat into the recipient sites creates the shape, volume, and structural changes defined in the operative plan. The fatty tissue should be deposited in the desired location, shape, and volume with each pass of the infiltrating cannula. The swelling will vary from patient to patient, from area to area, and even from side to side in the same patient.
Because all these visual clues seen during infiltration of fat can be deceptive, the intraoperative appearance of the infiltrated site should not be used as the sole criterion to determine the amount of fat to be placed, which is why it is important to estimate the volume to be infiltrated before the procedure begins.
IRREGULARITIES, LUMPS, CALCIFICATIONS, AND OIL CYSTS
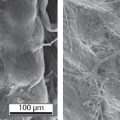
One of the most distressing and common outcomes with fat grafting is the presence of visible and palpable irregularities and lumps. These mainly result from necrosis of the grafted material. Kato et al 6 demonstrated that although a single dead adipocyte can be completely absorbed, the extruded oil droplets are replaced by a cicatrization phenomenon (collagen matrix formation), with chronic inflammation. If numerous tiny droplets (less than 1 mm) occur, palpable surface irregularities will develop. Should the necrosis be more consistent (greater than 10 mm), the formation of an oil cyst represents the typical evolution, leading to chronic inflammation. 7 Once established, oil cysts remain permanently, without any tendency to reduce in size or to resorb.

This patient presented with a left unilateral cyst on the jawline, resulting from fat grafting performed 1 year previously to correct facial asymmetry; 7 cc had been placed in multiple tunnels. The fibrotic cyst was noticed 1 month after surgery. No tendency to recur was noted after 1 year.

This woman’s bilateral fibrotic cysts resulted from fat grafting to correct tear trough deformity. The amount placed was 0.5 cc per side of refined less dense fat with a 19-gauge blunt-tipped cannula. To avoid a depression from excision of the cyst, a midfacelift was performed.
In critical areas, like the breast, the formation of oil cysts and calcifications may induce diagnostic problems with breast cancer 8 (see Chapter 42). However, calcifications resulting from fat necrosis are substantially different from those induced by breast cancer. An expert radiologist will be quite able to recognize the difference.
How Oil Cysts Occur
The likelihood of necrosis after grafting basically depends on the technique. Oil cysts are most often seen after large-volume transfer or bolus injection. They occur mainly in the breast and buttocks, where larger cannulas (16- to 18-gauge) are used; these are seldom used on the face. According to Kato et al, 6 the sequence is as follows: the death of adipocytes gives rise to oil droplets, followed by the formation of necrotic, calcified tissue, which eventually develops an oil cyst, with a tendency to grow. The solid wall around the cyst prevents absorption of new oil within the cyst itself, whose size and configuration will remain stable. 7
How to Prevent Oil Cysts
Placement of fatty tissue so that it creates a smooth fullness is imperative for a successful result. However, smooth placement demands that the physician have technical ability as well as experience and requires appropriate planning and determination of the appropriate volume to be injected. This is especially true in recipient areas with thin skin, as in the eyelid (see Fig. 52-3 and Chapter 23 for more discussion and treatment of these irregularities in the lower eyelids).
The use of thin cannulas (such as 21-gauge), less dense fat, a spaghetti-like aliquot technique, and painstaking molding of the grafted material provide potential solutions to overcome avoid fat necrosis, with unpleasant irregularities and oil cyst formation.
Related posts:
 Chapter 50 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE BODY
Chapter 50 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE BODY
 Chapter 49 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE FACE
Chapter 49 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE FACE
 Chapter 51 PERINEURAL FAT GRAFTING FOR THE MANAGEMENT OF NEUROMAS AND PAIN SYNDROME
Chapter 51 PERINEURAL FAT GRAFTING FOR THE MANAGEMENT OF NEUROMAS AND PAIN SYNDROME
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


