Chapter 49 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE FACE
The knowledge of specific fat compartments of the face has changed plastic surgeons’ understanding of facial aging and thereby the approach to facial rejuvenation. With our awareness of the existence of both superficial and deep compartments, it is now apparent that the aging process is largely the result of volume deflation, as so eloquently described by Rohrich and Pessa. 1 Volume loss occurs differentially within these compartments resulting in facial contour incongruity. This process has been called pseudoptosis, in which selective deflation of the deep cheek fat with age contributes to decreased projection of the superficial fat pads, resulting in an excess skin envelope and the illusion of ptosis. 2 , 3 This is in distinction to the youthful face, in which there is a smooth transition between compartments, resulting in an even, continuous contour.
Historically, the subcutaneous fat in the face was believed to be one confluent mass; therefore facial rejuvenation procedures were based on lifting and repositioning this subcutaneous tissue as one single unit with manipulation of the skin and SMAS. 4 The focus was primarily placed on the treatment of the SMAS and skin in varying vectors and degrees of tightening using techniques of SMASectomy versus SMAS plication. The evidence that this fat is compartmentalized, however, has allowed the development of techniques for differential restoration of facial volume in combination with rejuvenation through SMAS treatment. 5

To fully understand this mechanism, we must review various anatomic studies. 1 , 3 , 4 , 6 , 7 Their work elucidated a lattice of superficial and deep facial fat compartments discretely partitioned into multiple, independent units by fascial barriers.
Thirty hemifacial cadaveric dissections were performed following injection of methylene blue into specific regions; 18 male and 12 female cadavers were included, ranging from 47 to 92 years of age. 1 Findings included the following:
Nasolabial fat compartment: The nasolabial fat compartment is located anterior to the medial cheek fat and overlaps with the jowl. The orbicular retaining ligament (ORL) serves as its superior border. The nasolabial fat lies medial to the deep fat of the suborbicularis. The lower border of the zygomatic major is adherent to this compartment.
Cheek fat compartments: Cheek fat compartments include three components: the medial, middle, and lateral temporal–cheek fat compartments. The medial fat compartment lies lateral to the nasolabial fold, superior to the jowl fat and inferior to the ORL and lateral orbital compartment. The middle fat compartment is superficial to the parotid gland. The dense, fibrous abutment of the medial and middle fat compartments corresponds to the zygomatic ligament. The lateral temporal–cheek compartment is also superficial to the parotid and connects the temporal fat to the cervical subcutaneous fat. The lateral cheek septum is just anterior to this compartment.
Forehead and temporal fat compartments: This includes a central compartment in the midline and the middle compartments just lateral to this on the right and left. The previously discussed lateral temporal–cheek compartment then lies lateral to the middle compartments.
Orbital fat compartment: The orbital fat is composed of three compartments as well. These include the superior, inferior, and lateral. The ORL, which is a truly circumferential structure, acts as a boundary for these structures.
Jowl fat compartment: The jowl fat compartment adheres to the depressor anguli oris. The medial boundary is the lip depressor and inferior boundary is the membranous fusion of the platysma. It is important to note that this is separate and distinct from the nasolabial fat.
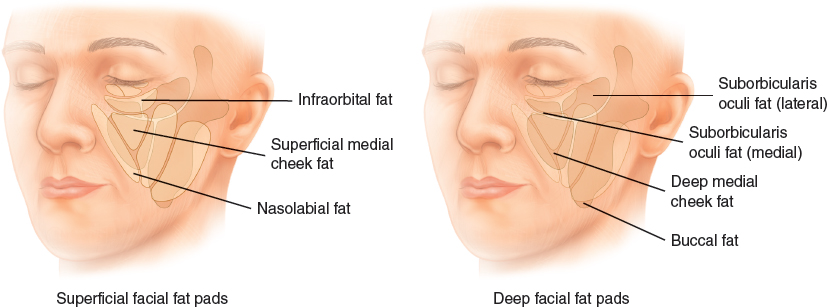
Deep layers exist as well, including the suborbicularis, retroorbicularis, and buccal fat pads. These fat compartments lie below and above facial muscles and enable sliding of these muscles during animation and mastication. 1 Although loss of deep fat is known to occur with aging in the temporal region, it is now known that this occurs in the deep medial cheek fat as well. 4 Further cadaveric anatomic dissections identified two areas of deep medial fat, both lying medial to the zygomaticus major muscle; the medialmost portion abuts the piriform and the lateral lies directly over the maxilla. 3 This deep fat compartment supports the overlying subcutaneous fat; loss of volume in this compartment results in a loss of anterior malar projection, a prominent nasolabial fold, and can create a V-deformity of the lower lid. Further studies have found that the fat in this deep medial cheek compartment also varies in size in comparison to the superficial compartments, more specifically the nasolabial compartment. The average adipocyte size is significantly larger in the nasolabial compartment than that in the deep medial cheek. 2 This finding may be partly a result of its location above muscles, its rich vascular supply, and the increased metabolic activity here compared with areas of deep fat, which are relatively inert and compressed against the skeleton, causing a relative atrophy. 2
The facial fat compartments are partitioned by a fibrous condensation of connective tissue, which originates from the underlying fascia to dermis and carries the perforator blood supply to the skin. 4 , 8 These fascial ligaments limit shearing forces on the face, thereby, creating a “retaining system” and provides stability for the vascular supply to the face. 4 , 8
These findings support the idea that facial rejuvenation should center on two key concepts: volume restoration and facial recontouring. This is not a new concept; Ristow described direct injection of autologous fat directly into the deep cheek fat in 2001. 3 , 9 Effects are immediate, resulting in improved anterior projection, decreased nasolabial fold, and corrected V-deformity of the lower lid creating a youthful cheek and lid-cheek junction. 3 Fat augmentation into these specific compartments allows for an increased ability to precisely restore facial volume with improved control and precision. The most important and relevant fat compartments in facial rejuvenation include the deep malar, the deep nasolabial fat compartment, and the superficial middle and lateral (high) malar compartments. 10 This can be performed separately in young patients with minimal skin excess and laxity or as a complement to tissue lifting through the manipulation of the skin and SMAS. 5 The synergistic effects of fat grafting of the specific facial compartments mentioned above and SMAS manipulation through SMAS-stacking or SMASectomy was evaluated in a recent review by Rohrich et al. 5
Patients and Methods
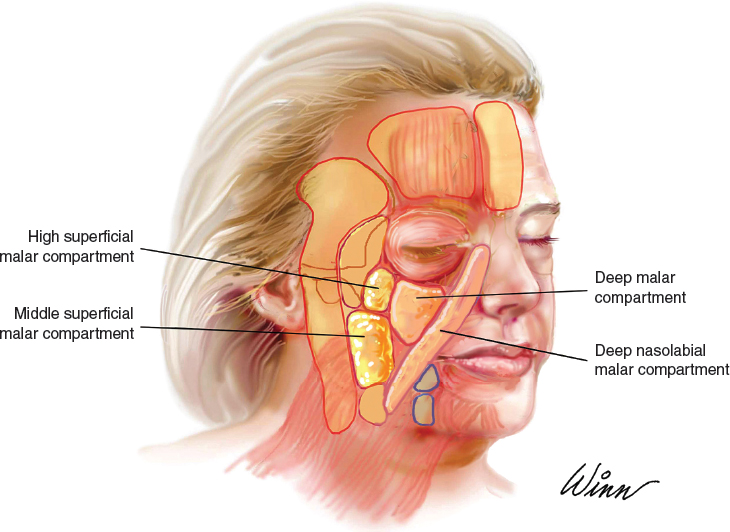
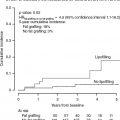
A retrospective review was performed of all patients undergoing the lift-and-fill technique by the senior author (R.J.R). The technique includes individualized component facelift as described previously, 10 open neck lift, fat transfer to the deep malar fat compartment, nasolabial folds, and superficial middle and high malar fat compartments, and facial resurfacing if necessary. Key fat compartments relevant to the lift-and-fill face lift are shown above. Typical volumes of fat were 1 to 3 cc injected into each compartment with the average transferred volume being 2 cc per compartment. Typically, the fat was harvested manually from the abdomen or thighs using a 10 cc syringe and cannula. Once prepared, the fat was allocated into 1 cc syringes and injected directly into these fat compartments using a 19-gauge needle. Care is taken to aspirate before injection to ensure the fat is not injected directly into a vessel. The total average injectate per face was 12 cc (range 8 to 14 cc). The 100 consecutive facelift patients who also underwent simultaneous fat compartment fat grafting (96 women and four men) were then analyzed using a computer-based system to evaluate certain data points. Inclusion criteria were at least 6 months postoperative follow-up and a position-matched oblique photograph between preoperative and postoperative imaging.
Complications that were assessed were divided into minor and major subgroups. Major complications included any event that resulted in a surgical revision or return to the operating room. Minor complications were all those managed conservatively.

Outcomes were evaluated using contour ratios of specific facial points. Clinical assessment included the degree of preoperative and postoperative change of the nasolabial fold depth as described by Barton 11 and the two-dimensional location change of the most-projected malar point on an oblique photograph. Point A represented the most-projected malar apex, and point B showed the submalar concavity. All distances were divided by the interpupillary distance to determine a ratio. A computer software program was created to quantify variations in these facial landmarks, as previously described. 12 Data from digital images were analyzed based on three variables: x- axis, a horizontal line intersecting the midpupil; y- axis, a vertical line drawn from the midpupil on the side of face to be measured, and interpupillary distance. The lateral contour of the face was then outlined, and points A and B were identified manually. The program then generated the location of points A and B as an x- and y-axis value.
A negative variation on the x-axis corresponded to a decrease in lateral contour projection, whereas a positive variation denoted an increase in volume and projection. Likewise, a negative variation of the y-axis corresponded to a lowered vertical displacement of projection, while a positive variation resulted in a higher position of the most-projected point, meaning that the point was moved vertically through the lifting of the skin and SMAS.
Finally, a pair of plastic surgery observers evaluated preoperative and postoperative photographs and graded the nasolabial fold (NLF) and malar eminence in each case. NLF scale: 0, No visible fold; 1, minimal; 2, moderate; 3, very deep fold. Malar score: 1, Concave with projection below zygoma; 2, neutral projection; 3, convex malar projection below the zygoma.
Related posts:
 Chapter 50 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE BODY
Chapter 50 ANATOMY AND HISTOLOGY OF THE FAT COMPARTMENTS OF THE BODY
 Chapter 51 PERINEURAL FAT GRAFTING FOR THE MANAGEMENT OF NEUROMAS AND PAIN SYNDROME
Chapter 51 PERINEURAL FAT GRAFTING FOR THE MANAGEMENT OF NEUROMAS AND PAIN SYNDROME
 Chapter 52 COMPLICATIONS
Chapter 52 COMPLICATIONS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


