Chapter 46 AESTHETIC LIPOSCULPTING AND FAT GRAFTING FOR THE BUTTOCK AND TORSO
Today fat grafting is quickly becoming the benchmark procedure for buttock contouring as well as for large-volume muscle enhancement of the calves, pectoral muscles, rectus abdominis muscles, biceps, deltoids, and other anatomic areas. Fat has gone from being one of the most underappreciated body components to one of the most valued because of the potential role it plays in large-volume expansion and restorative and regenerative medicine. Fat grafting is my preferred method for gluteal augmentation/reshaping. It provides greater versatility, precision, and selective augmentation, with a shorter recovery period and fewer complications than gluteal implants. The challenge at times is recognizing whether enough fat is available for harvest.
Material and Methods
INSTRUMENTS AND EQUIPMENT
When I first began performing fat grafting 15 years ago, little was understood about gluteal aesthetics, and there were few technologic devices to support the gluteal fat grafting procedure. Instruments were quite simple, consisting of a harvesting and injection cannula, strainer, collection bottle, and syringes. Finding the right collection system and instruments was a tedious process; various manufacturers and suppliers had to be sought to assemble these simple instruments. Today it is much easier to find the needed instruments, but liposuction equipment has become more complex, with a number of different technologies to help with fat extraction: internal and external ultrasound, power-assisted machines, radiofrequency applications, laser devices, and other modes. Thus the surgeon has many options to facilitate the liposuction and fat grafting process. This equipment can be costly, so each surgeon must decide which devices will be beneficial in time saved and improved outcomes to justify the expense.
I currently use the following technologies:
Power-assisted liposuction (MicroAire) machine
Autoinjection power-assisted Wells Johnson fat transfer machine
Box 46-1 Overview of Approach to Fat Harvest and Preparation
My harvesting approach employs the following:
Larger-bore cannulas for fat harvest: 5 mm cannula
Power-assisted liposuction in every case
Closed Wells Johnson reinjection system
Power-Assisted Liposuction
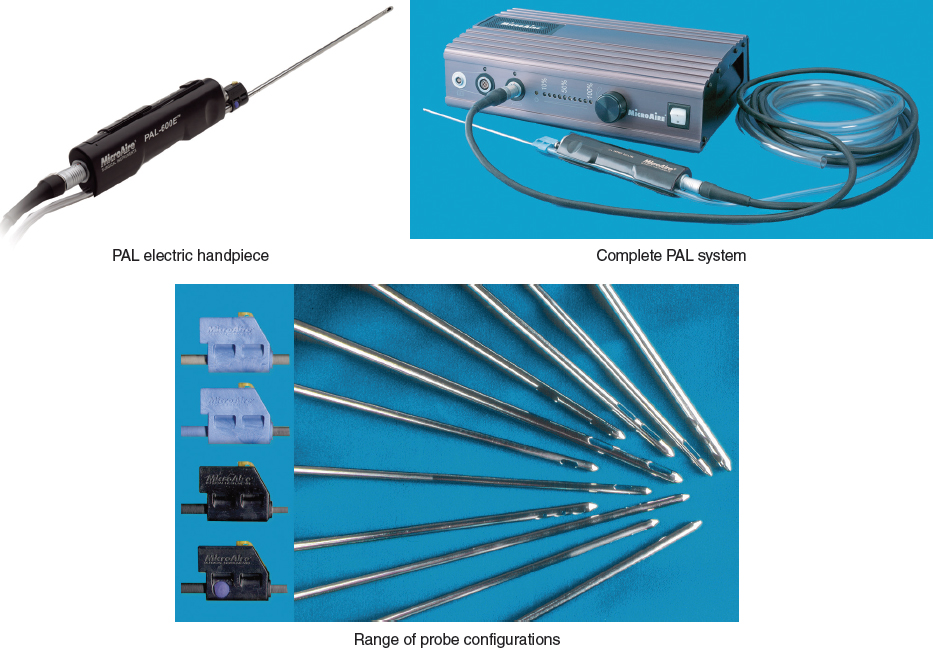
I perform all my cases with a power-assisted liposuction (PAL) machine (MicroAire, Charlottesville, VA). This equipment has an electrically powered reciprocating cannula (4000 to 6000 cycles per minute) that makes suctioning much easier and less tiring for the surgeon. The machine works quite well and speeds up the liposuction process. The system does not use heat; however, if the operator is not careful, friction skin burns can occur that will not be detectable for at least 2 to 3 days after surgery.
In my experience with the PAL system, it does destroy about 10% of the harvested fat, but this is a tradeoff that I am willing to accept, since the benefits far outweigh the 10% loss.
The Wells Johnson Auto-Graft Injection Closed System

My current fat collection, fat preparation, and reinjection system consists of a 2 L canister from Wells Johnson (Tucson, AZ). These are very large Lukens trap devices that collect the lipoaspirate.
There have been significant advances in the field of fat grafting. One of these is the ability to autoinject the fat through a closed pump system using the same aspiration cannula that was used to extract the fat (a 5 mm basket cannula). This has revolutionized my grafting technique, sped up the process, and removed the issues I had with the open system, in which fat was exposed to air, increasing the potential for contamination of the lipoaspirate, and there was loss of small particles of fat (about a 15% to 20% loss of fat cells through the straining process I was using to prepare the fat). This system has greatly decreased the time consumed in preparing the fat, so I have replaced my old syringe-and-strainer process with this closed system.
The drawback to the reinjection decanting system is that I cannot get rid of all of the fluid that is in the lipoaspirate, so the injectate tends to have a higher water/fluid content (about 20% more) than with my old method of straining. This means that I will have a false higher absorption rate, since there is more fluid in the transferred fat. However, I am preserving the smaller fat cells that I formerly lost through the strainer (about 20% fat lost).
PREOPERATIVE PREPARATION
All procedures are performed with the patient under general anesthesia in my officebased surgical center (ASA 1 and 2 patients only). The surgical team is small: the anesthesia provider, the circulator, my surgical assistant, and me.
Evaluation and Laboratory Tests
Routine preoperative medical evaluation and laboratory tests appropriate for age are performed. The patient is instructed to stop taking all medications and products that affect platelets at least 2 to 4 weeks before treatment. Bowel preparation agents are not routinely given. Patients who have rheumatoid arthritis and are taking immunosuppressive medications such as infliximab (Remicade) may be more susceptible to infections, including Mycobacterium infections, 1 so these medications should be stopped at least 2 weeks before the procedure and discontinued for 1 to 2 months thereafter. The patient is made aware of this increased risk of infection, and a clearance from their rheumatologist is obtained.

The morning of surgery, the patient is photographed. This must be a three-dimensional procedure: every aspect of the buttock will look different from different angles, so it is important to capture these views preoperatively. This also allows the surgeon to discuss the areas to be treated with the patient. The patient is asked to rotate a full 360 degrees, using quarter turns, so I can capture the front and back from a variety of angles. Nine photographic positions are used, including the “diver’s” position, to assess the triangular lower gluteal crease zone.
Markings
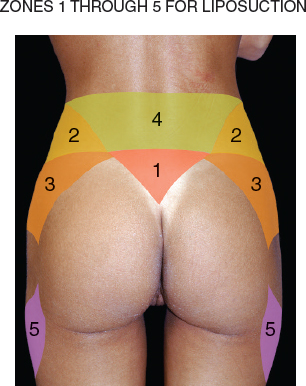
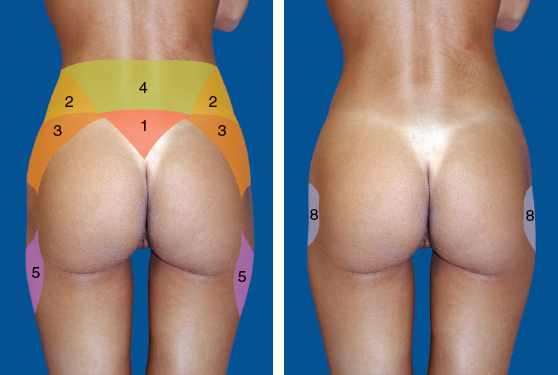
Also on the day of surgery, in the holding area, the patient is marked while standing. The areas to be liposuctioned are identified; these always include zones 1 through 4 and the areas over the oblique zones. 2 Zone 5 has cultural ramifications: some patients desire fat added in that area, whereas others request that fat be removed from this region.
Although there are 11 aesthetic units to the posterior region, there are 6 important zones that truly define the buttock frame and shape (zones 1 to 5 and zone 8) that I will discuss here.
The patient is reminded that in our state (Florida) we have a 4 L supernatant fat limit, and therefore it is possible that not all the areas being marked will be suctioned. Markings of these areas are in case I need to harvest more lipoaspirate. My main focus and priorities are zones 1 through 4. If more fat is needed for reshaping, I turn to the outer aspect of the legs (zone 5, if excess is present), abdomen, inner legs, inner knees, lateral chest wall, and in extreme cases, the arms, until enough fat has been obtained for fat grafting, staying within the 4 L limit and my comfort level.
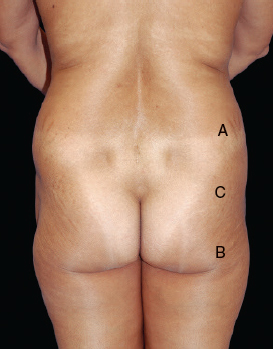
Three landmark areas are identified in the buttocks:
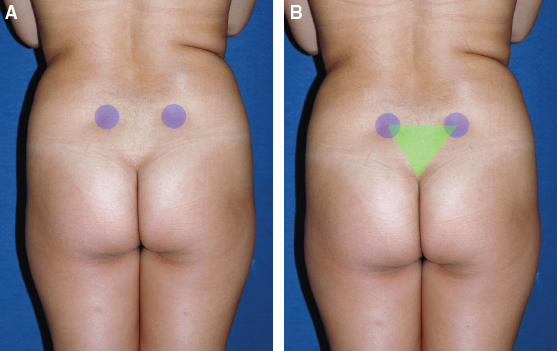
The first is the posterior superior iliac spine (dimples in the parasacral areas); this represents the height of the gluteal muscle I am trying to achieve.
With these points marked, it is easy to identify and mark the V zone (zone 1). This is the presacral space, identified by the superiormost point of the intergluteal fold and both posterior iliac spine dimples. Connection of these points creates a V, which is zone 1. When this zone is suctioned, it adds significant aesthetic contour to the buttocks.
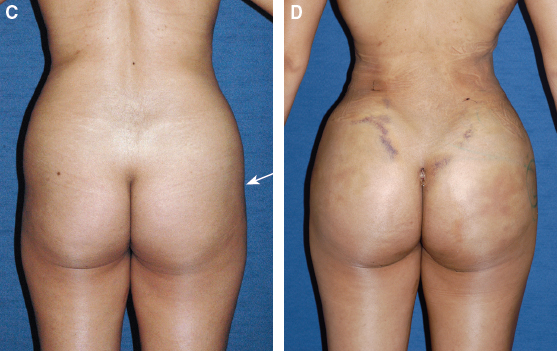
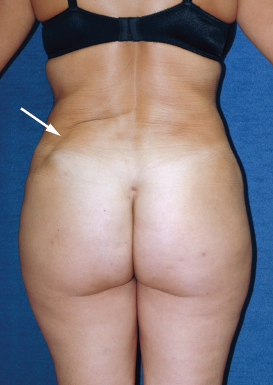
Any depressions in the midlateral buttock (white arrow, zone 8) are identified.
Sometimes these depressions extend all the way to the anterior leg. Therefore care is taken to mark the lateral extent of the deficiency, and any dimples or irregularities are marked. Zone 3 is evaluated and an attempt is made to quantify the amount of fat to remove: very little, none, or a lot. The markings are photographed; these photos become extremely helpful during the procedure, because the marks are often erased during surgery.
Medications
Before the procedure begins, 1 L of intravenous fluid is administered. Preoperative medicines given include clindamycin (Cleocin) 600 mg intravenously. If the patient is at high risk for postoperative nausea, ondansetron (Zofran ODT [orally disintegrating tablet]) 8 mg is given sublingually before surgery. Dexamethasone (Decadron) 10 mg is given intravenously toward the end of the procedure to reduce postoperative swelling and to help prevent nausea and vomiting. If the patient has a history of reflux, metoclopramide (Reglan) 10 mg and ranitidine (Zantac) 50 mg are added intravenously, especially since the patient will be lying in the prone position.
Operating Room Preparation and Initial Patient Positioning
With below-the-knee TED hose and pneumatic stockings in place, the patient is prepped circumferentially while she is in the standing position with room-temperature Hibiclens or Betadine solution.
Patient Positioning on the Table
The patient is now ready to be placed supine on the operating table; her arms are kept above the head while one assistant continues to keep all the tubing out of the way and the other assists her in lying down by holding her leg and supporting her upper back. The patient is asked to gently lie down; she is then asked to place her arms on the arm boards. The pneumatic tubing is kept inside the stockings.
At this point, the pneumatic stocking compression tubing is brought out and connected. It takes two assistants to do this: one remains sterile while the other connects the tubes.
All pressure points are padded. The patient is then covered, and induction of anesthesia may begin.
Following induction, and with the assistant prepared and gowned using a new set of sterile gloves, a Foley catheter is inserted. The patient will be going home with the Foley catheter still in place so that she does not have to get up every hour to urinate. This feature becomes extremely convenient for the patient; the catheter also helps in monitoring fluid status. The catheter is removed the next day, during her follow-up appointment. The patient is once again prepared with precautionary measures, and the infiltration process begins.
TECHNICAL GUIDELINES
Tumescent Fluid Mixture
The fluid mixture that I use is composed of the following:
1 L of lactated Ringer’s solution
25 ml of 1% lidocaine
Epinephrine 1:100,000 (1 ampule for the front but when working hard dense back and waist areas, I add 2 ampules)
Box 46-2 Reference Values When Using the Tumescent Approach
4 to 5 L of tumescent fluid usually injected
4 to 5 L of intraoperative intravenous fluids used
5 to 6 L of lipoaspirate (fluid and fat) required to obtain 2 to 3 L of supernatant fat
Harvesting

The areas from which I harvest fat depend on the amount of the patient’s available fat, as identified preoperatively, and the amount of fat needed for contouring, reshaping, and augmentation.
Harvesting by Zones
My goal is to reshape and recontour the body frame; therefore fat will be removed from areas that will accentuate the entire gluteal zone. In almost every case, regardless whether fat or implants are used for volume expansion, I perform liposculpting of zones 1 through 4. Zone 5 requires less suctioning. As noted previously, this zone carries cultural significance; some patients feel very strongly that they want to preserve the contour of this area, whereas other patients request reshaping of this zone.
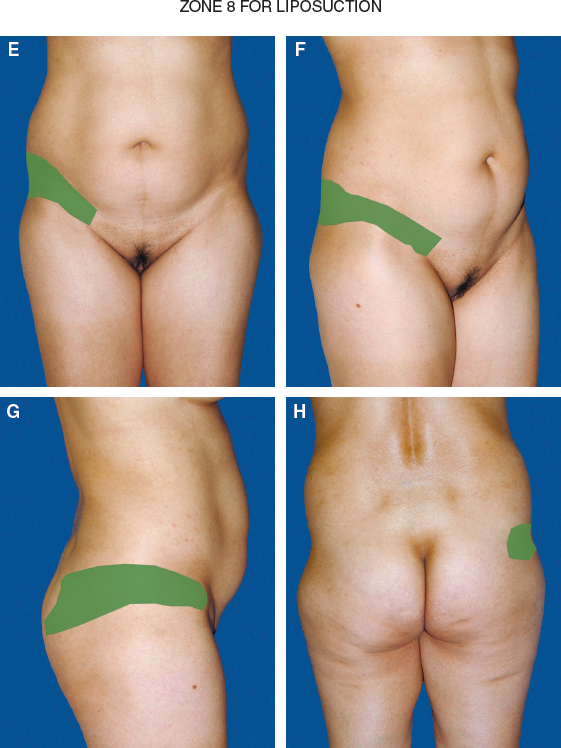
The midlateral buttock (zone 8) is of particular interest, because it is the only zone out of the 6 that may require fat grafting to smooth the contour. This zone has no muscle; therefore fat grafting will be to the less vascularized subcutaneous tissues and will require more care and precision with the grafting technique.
What other areas will be contoured depends on the amount of fat present. In large- or extra-large-framed individuals, because I have a state-imposed 4 L supernatant fat extraction limit, my goal is to shape the waist and frame, so I may be limited in suctioning other areas, such as the abdomen or back. The patient is advised of these limits.
However, if the patient has a small to medium frame, I contour the abdomen first, then the waist and frame, and then move on to other areas: the lateral chest wall, upper back, inner legs, inner knees, and perhaps the arms.
Selecting the Harvesting Technique Based on Fat Characteristics
My harvesting technique varies, depending on the patient’s presenting fat characteristics and available fat. I usually start the procedure by introducing a 5 mm cannula into the deep layers. This allows me to assess the characteristics of the fat that I am about to extract and answer the following questions: Is the fat hard or soft? Does it extract quickly or slowly? Is it difficult to extract, or does it come out like butter? Does it have a propensity toward leaving surface irregularities? Is the superficial layer thick or thin, compact or loose? Can the deep layer be easily distinguished from the superficial layer, or does it all seem to blend in?
From the results of my assessment, I adjust my approach and technique. If the patient has extremely dense fat, in that particular dense zone I pre-tunnel (using the power-assisted cannula) to help soften the fat (this is usually in the upper and lower abdomen and linea alba/midline). This is the Simeon Wall, Jr., technique called “SAFE” Lipo (separation, aspiration, equalization).
Liposuction is performed with the patient in the supine, lateral decubitus, and prone positions. Each position has a specific purpose and technical goal that has become more apparent to me as I have learned to contour the body and buttock areas.
The supine position is used to address the following areas:
The abdomen
The zones overlying the external/internal oblique zones
Some of the posterior triangle
The lateral chest wall
The inner legs (if needed)
The abdomen is contoured, but this does not affect the buttock frame or gluteal contour; it is merely a fancy harvesting approach. However, when contouring in the supine position, it is important to avoid accidently disrupting the frame shape.
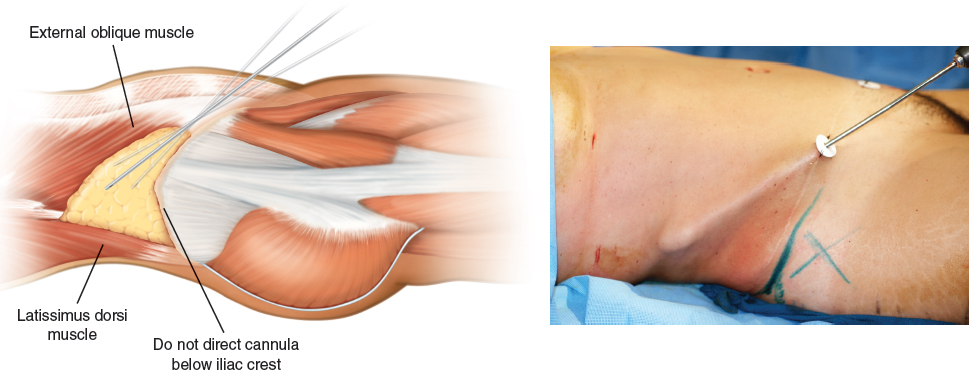
While the patient is in the supine position, the surgeon should avoid suctioning below the iliac crest (marked by an X in the photo). This zone below the crest corresponds to point A on the frame.
If this small technical point is not followed, oversuctioning of the upper buttock may occur, creating a step-off that does not flow smoothly.
The areas below the iliac crest and zone 3 (white arrow) should be suctioned under direct vision with the patient in the lateral decubitus position.
Contouring
Lateral Decubitus Position
Contouring of the gluteal frame and gluteal zone begins with the patient transferred to the lateral decubitus position. The following areas will be treated:
Aesthetic unit 2: The posterior flank triangle; the waistline
Frame point A: The upper lateral buttock
Zone 3
Frame point B: The outer legs, if needed
The posterior lateral chest wall zone and back
Aesthetic Unit 2 Contour
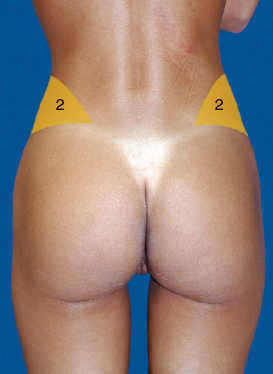
Setting up the gluteal frame is performed by creating a smaller waist. To help create a smaller waistline, suctioning of the lower back and sacrum are needed, but the most important zone is the posterior flank triangle, aesthetic unit 2. These areas begin to set up the aesthetics of the frame shape and are best approached with the patient in the lateral decubitus position.
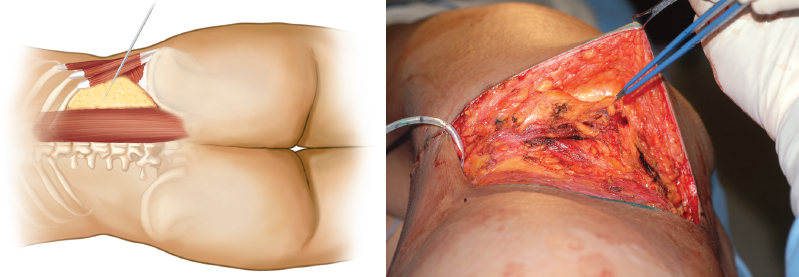
The posterior flank triangle is defined inferiorly by the superior iliac crest, superiorly by the twelfth rib, medially by the lumbar muscle, and laterally by the internal oblique muscle (left, above).
A very distinct fat pad exists in this triangular zone. This fat pad is highly movable and tends to shift around when the patient is placed in different positions, thereby giving the illusion that the fat has been completely suctioned, whereas in reality it has shifted.

To truly contour this fat pad zone, the surgeon must approach it not only with the patient in the lateral decubitus position but also in the prone position. In the past, I tried addressing the waistline when the patient was supine and prone, but the contour was never really as refined as desired. It looked good while the patient was on the table, but the results 3 to 6 months later left something to be desired.
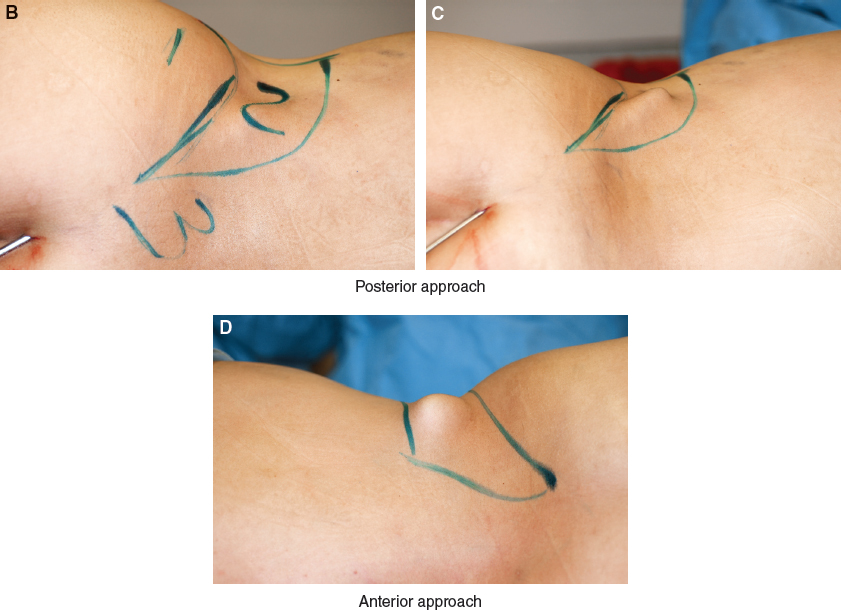
It was not until I learned how to really suction the posterior triangle in the lateral decubitus position that I started to see tremendous changes. This area requires a three-dimensional approach. It is started with the patient supine, then the patient is transferred to the lateral decubitus position and suctioning continues. However, these positions alone will not be sufficient to achieve the result I am seeking; the posterior triangle also has to be suctioned with the patient in the prone position.
Related posts:
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 48 LOWER EXTREMITY RECONSTRUCTION
Chapter 48 LOWER EXTREMITY RECONSTRUCTION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


