Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Liposuction is one of the most commonly performed surgical procedures in the world. Coleman structural fat grafting is an essential tool for all aesthetic surgeons performing liposuction, because it provides the key to addressing iatrogenic liposuction deformities, the most common complication of liposuction.
Patients with deformities resulting from liposuction were the first patients in my practice (S.R.C.) on whom I attempted fat grafting, so they are the patients with whom I have had the longest experience.
Unlike the use of fat to rejuvenate the hand, successful treatment of body surface irregularities requires a three-dimensional visualization of the problems and solutions.
Aesthetic Considerations
Liposuction makes it possible for surgeons to change a patient’s corporeal proportions much more easily and safely than open surgical procedures would. With the introduction of liposuction in the early 1980s, women can have their thighs, abdomens, and arms selectively contoured to rid themselves of “saddlebags,” large buttocks, abdominal bulges, and hanging arms. Buttock creases can be recarved to create “smiles” under the buttocks. In a relatively short time after its arrival, liposuction became one of the most commonly performed surgical procedure in the world. As liposuction developed in the late 1970s to the mid-1980s, a new clinical entity, the postliposuction iatrogenic deformity, made its appearance. Any surgeon who performs liposuction will confront liposuction’s most common complication: superficial surface irregularities. Some of these are exaggerations of preexisting irregularities, some are cellulite, and some are newly created. The thigh and abdomen are particularly prone to irregularities, and physicians have come to accept such indentations as an acceptable outcome of liposuction.
However, postliposuction iatrogenic deformities are not just limited to surface irregularities. Changing the relationship between a woman’s thighs, hips, and abdomen can result in an unnatural and even bizarre proportion. For instance, a dramatic decrease in the size of a woman’s lateral thighs without an appropriate decrease in waist size can result in a boxy and even masculine appearance. Flattening the lower abdomen without attention to the upper abdomen can add to this boxy appearance. Minor reductions in the volume of the buttock and/or lengthening and deepening of the buttock creases interrupts the continuous flow of the lateral and posterolateral thigh into the buttock. Such maneuvers often create a buttock that would be considered unattractive if it occurred naturally.
In 1987 I began treating iatrogenic liposuction deformities with fat grafting, primarily focusing on surface irregularities. As I became more proficient at fat grafting, I began to address corporeal proportion to restore a more natural aesthetic proportion after liposuction and to reestablish a feminine relationship between waist, hips, and thighs.
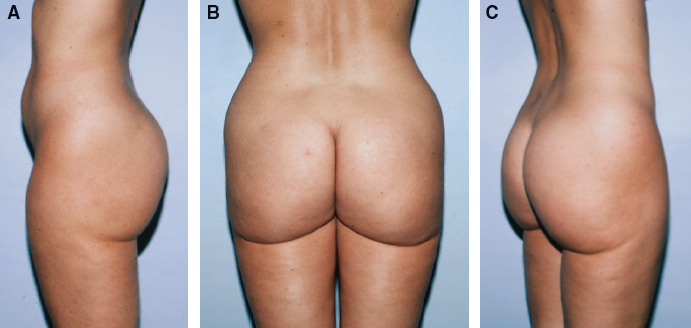
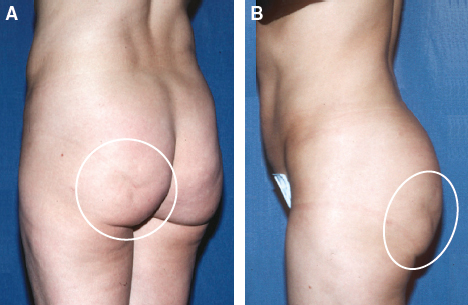
This 30-year-old woman presented 2 years after liposuction had been performed on her lateral thighs, buttocks, and love handles. She was distressed because the deepening of her buttock crease now wrapped around her thigh. She felt that her legs looked shorter and her buttocks bigger and more ptotic after the procedure. She also noticed that her body appeared “boxy” and less feminine. When she complained to the plastic surgeon about the appearance of her buttocks, she discovered that he had deliberately deepened her buttock crease to make it more “aesthetic… smiling.”
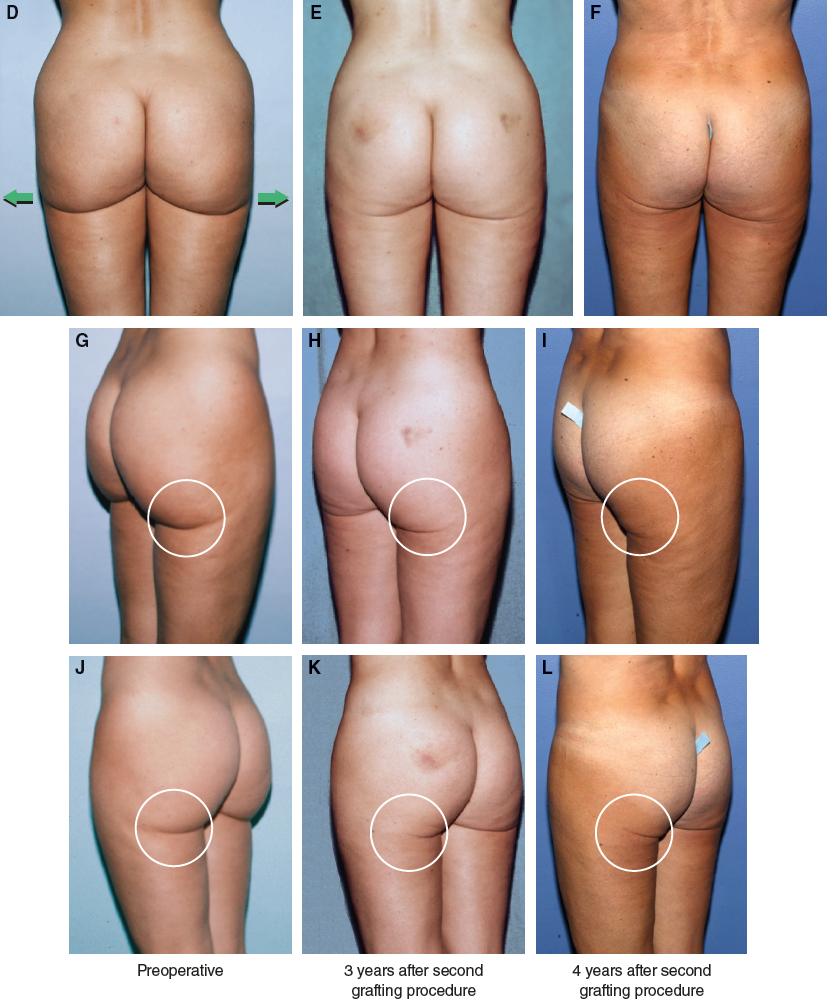
The patient is shown 3 and 4 years after her second procedure to restore a more normal appearance to her body. Fat was harvested from her waist, upper hip, and lateral buttocks then placed into her buttock creases and lateral thighs to create a more feminine and natural relationship among the waist, hip, and thigh.
By filling in the deepened buttock crease and slightly expanding the thighs, a more normal buttock-thigh interface was reestablished. By restoring the continuous flow of the buttocks into the thighs, a more attractive and youthful line of the leg is restored.
Restoration of this buttock-thigh interface can have profound effects on the appearance of the lateral thigh, with smoothing of apparent irregularities.
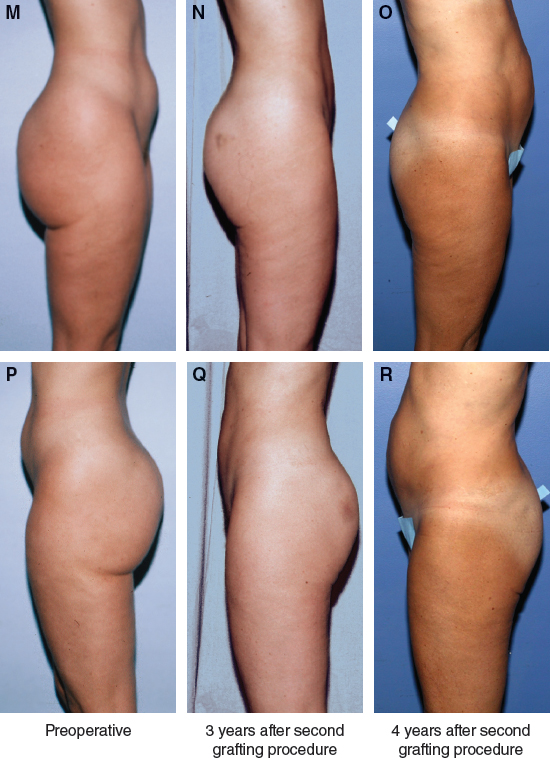
Expansion of the thighs and buttock creases creates the illusion of a vertical lift. However, the vectors are radial. Restoring the continuous flow of the buttocks into the thigh produces a more attractive and youthful leg contour.
Liposuction is a powerful tool for alteration of the proportions of the body, but the consequences of removing elements of the body or adding artificial elements must be recognized. Careful planning with a clear vision of the overall result is paramount for aesthetic excellence.
Patient Selection
Patients who present with corporeal iatrogenic deformities have usually had negative experiences with aesthetic surgeons. How they perceive themselves is colored by those experiences, so it is often difficult to assess how realistic the patient is about his or her current appearance as well as his or her expectations.
The surgeon should not agree to perform a correction unless he or she is reasonably confident that the patient’s deformity can be rectified. The patient should be clearly told that new deformities may be created by harvesting fat to correct the existing irregularities.
The surgeon must have a reasonable expectation that a positive correction of the patient’s deformity can be accomplished without creating unacceptable new problems (such as donor site irregularities or deformities). Furthermore, the surgeon should believe that the positive correction will be demonstrable on photographs and that the patient will be able to appreciate the positive change.
It is never productive to be disapproving of surgeons who previously performed surgery on a patient, because these patients usually already have critical feelings about their previous procedures. If the corrective surgeon contributes negative dialogue to the consultation process, the feelings of pessimism experienced by the patient can be exacerbated. This can make it very difficult for the surgeon to ultimately satisfy the patient. Care should be taken to approach future procedures constructively; I hesitate to operate on a patient who has a negative attitude about the planned procedure.
Material and Methods
TECHNICAL GUIDELINES
Anesthesia
In the past, epidural or occasionally general anesthesia was used for these procedures. However, in an effort to minimize complications, my anesthesiologist now most commonly uses total intravenous anesthesia (TIVA) for these procedures. I am fortunate to work with an anesthesiologist who is highly experienced with officebased surgery and administering this type of anesthesia, which consists mainly of propofol, ketamine, and a narcotic agent. The benefit of this type of anesthesia is that patients awaken rapidly, even after prolonged procedures, which are not uncommon when grafting large volumes of fat for extensive deformities. In addition, postoperative nausea, lightheadedness, and grogginess, which can occur with inhalant anesthesia, are rarely experienced.
In addition to TIVA, local anesthetic is also used in both the donor sites and the areas to be infiltrated. Harvesting sites are infiltrated with the same mixture of lidocaine, epinephrine, and lactated Ringer’s solution as the sites to be grafted. The mixture consists of 50 ml of 1% lidocaine and 1.25 ml of epinephrine 1:1000 for every 500 ml of Ringer’s lactate solution. The harvesting sites are infiltrated with a 1:1 ratio of wetting solution to volume of lipoaspirate.
Incisions
When harvesting from the back, sacrum, or hip, the lateral sacral depressions are used as the main incision sites. Incisions into the sacral depressions are much better tolerated than incisions anywhere else in this region, because the resulting incisional scar is less visible, even if it does become depressed or pigmented. Occasionally an incision in the midline over the spine is used as well. This allows for suctioning to take place from two different directions. When harvesting from the inner thighs, a groin crease incision is made. Incisions that are 2 mm long are placed around the recipient sites to allow fat placement from at least two directions.
Harvesting and Fat Preparation
Harvesting sites are selected to enhance body contour, as there has been no clear correlation between donor site location and longevity of the implanted tissue. Care must be taken to minimize the amount of fat suctioned from any one area such that new deformities are not created. Incisions are made with a No. 11 blade scalpel, and a blunt Lamis infiltrator is used to infiltrate the previously described wetting solution. The harvesting cannulas are Coleman aspiration cannulas, which have been designed to minimize trauma to the tissue to be grafted. Only a minimal amount of negative pressure is applied by hand to the 10 cc syringe to which the cannula is attached, again to minimize damage to the parcels of fat.
After harvesting, the cannula is removed from the syringe and replaced with a cap, and the plunger of the syringe is removed. The syringe is then placed into a sterilized sleeve and centrifuged for 2 minutes at 1200 g. The oil layer is decanted, and then the aqueous component is drained.
Infiltration Cannulas
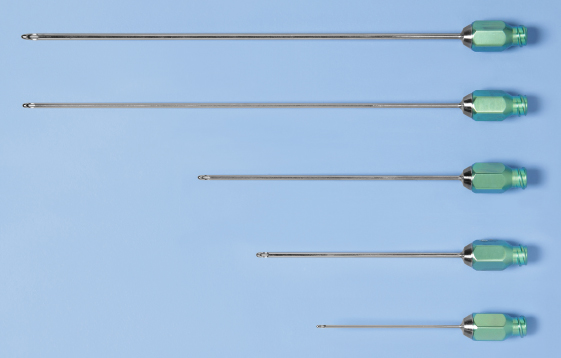
I connect 3 cc syringes to the longest Coleman cannulas, which are 14- to 16-gauge and vary in length from 7 to 15 cm. I prefer to use the shorter cannulas (usually 9 cm), but to avoid too many incisions, I will switch to a 15 cm cannula so I can extend placement from any one incision. When using a 15 cm cannula I prefer to use one that is thin, but controlling the longest cannulas through fibrous planes can be difficult, so I switch to a 16-gauge cannula if there is much resistance. I alternate between straight and curved cannulas, depending on the curvature of the underlying structures. Although I have some cannulas with more dramatic curves, I frequently will bend the longer cannulas to create a gentle curve to follow the body, such as in the back or thighs. Although cannulas with the curve prefabricated into the shaft can be helpful to navigate curvatures of the body, the new multiholed cannulas are slightly bendable. These can be adjusted to create a curved plane.

I fill the syringes with 2.5 cc of processed lipoaspirate to make them easier to manipulate. Unlike the 1 cc syringes, these syringes can be reused repeatedly without the plungers sticking. The technique of placement in the body differs from that described for the face and hands in that slightly larger amounts are placed with each pass. However, even for a long pass, no more than 0.5 cc is ever intentionally placed in a single withdrawal.
Level of Infiltration
The level of infiltration depends on the desired outcome. To accomplish large contour changes to the thighs or buttocks, fat is layered into the deep planes. In those deeper fat planes and especially if any tissue is placed into muscles, the thicker 16-gauge 15 cm type I cannulas are used. The blunt large cannulas minimize the possibility of damage to vessels and nerves in the muscles.
For a specific groove or depression, more tissue is placed superficially. Placement should be perpendicular to the grooves or depressions that are more linear in nature. This helps to prevent the creation of a sausagelike deformity, which can occur if fat is placed only in a direction parallel to the long axis of the depression. To address superficial problems, placement starts immediately subcutaneously and infiltrates layer by layer to a deeper plane, specifically feathering as the placement deepens.
Volume Ranges
Volumes for correction of corporeal deformities vary from 1 cc placements into minuscule irregularities to as much as 300 or 400 cc into a deficient thigh, buttock, or arm. Experience and accurate photographs are the most valuable tools for determining accurate volumes. The amount of fat harvested is twice as much as the amount estimated to be used for grafting.
TECHNIQUE
Key to Technique
The most important step in correcting corporeal deformities is analysis of the defect. If the surgeon cannot adequately demonstrate a deformity on film, it will be almost impossible to show that the procedure resulted in a positive change.
Photography for corporeal proportion is relatively standard and needs little explanation, but photographic techniques to demonstrate surface irregularities are generally inadequate. Casual observation and commonly practiced conventional photography will not clearly define the problem in a manner that reveals the deficiency, especially to the degree that the patient sees it.
When a patient sees her body in a standard photograph, she will usually say that the photograph does not accurately portray the full extent of the surface irregularities that she sees when she looks at herself unclothed. The primary reason for this discrepancy is that the patient is most often looking down at her body with downward lighting when she sees these irregularities, whereas standard photographs are taken without this elevated perspective and with more diffuse light. As a result, it is difficult to appreciate the patient’s deformity with the standard views that plastic surgeons routinely take.
For example, with this patient, standard photographs provided scant evidence of the large depression in the left buttock that the patient complained of.
In an effort to address this discrepancy, I tried to photograph the patient with down lighting, up lighting, side lighting, and with the patient in many physical positions, but with little success. I finally developed a system of photography for analyzing corporeal defects to more accurately reflect what the patient perceives and desires to have corrected. Several years ago, one of my patients insisted that I take photographs of her body while I was standing on a stool so that the camera was a few feet above her. From this “bird’s-eye” perspective we were both able to appreciate the extent of her corporeal surface irregularities much better than from any of the standard views.
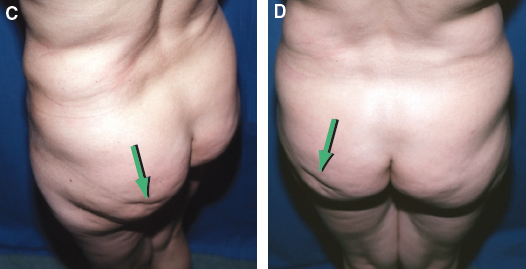
With this bird’s-eye view of the patient, the defect in the left buttock is clearly visible in the same way that it is visible to her as she looks over her shoulder or in the mirror with down lighting.
Even large irregularities can be difficult to discern in the normal photograph compared with the bird’s-eye view. I now stand on a stool and take about ten views of a patient’s body for almost any corporeal procedure that I perform. This angle allows me to appreciate the patient’s surface topography much more clearly than with the photographic techniques I used to use. By shooting a patient from a bird’s-eye view I am better able to see the problem that the patient wants corrected.
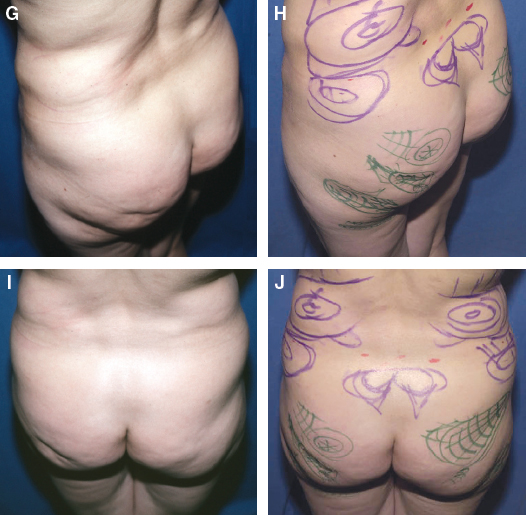
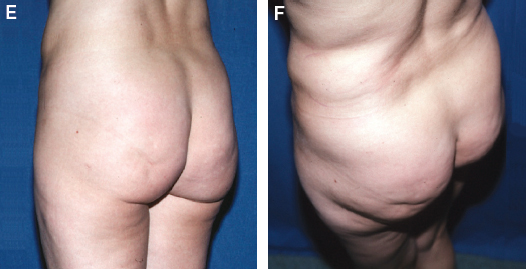
After the patient is marked to demonstrate which areas will be harvested and where the structural fat will be placed, I photograph the patient. Before the procedure begins, I compare the marked and unmarked photographs, both with the patient standing. The photos are placed side by side so I can more accurately determine the relationship of the marks to the actual deformity while I am operating and the patient is lying in a supine or prone position.
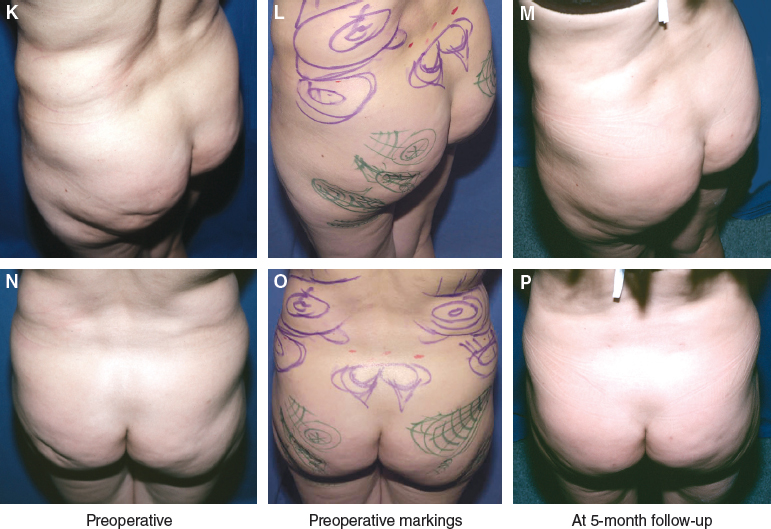
Clear photographic visualization by the surgeon of the extent of the patient’s defect is essential for making a plan and evaluating the extent of correction. This photographic maneuver gives me a standardized method of evaluating my results so that I can better appreciate the volumetric changes in my patients. These bird’s-eye views allow the surgeon to better understand the effect that volume changes have on the body’s shape.
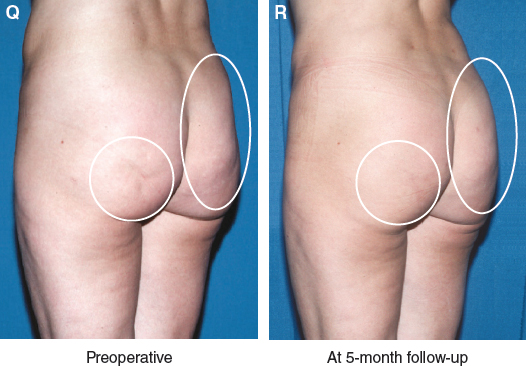
The fat grafts have reshaped the buttock to almost provide a “lift” to the upper buttock.
Being able to review the bird’s-eye photographs while I am transplanting fat into the areas has proved very valuable. The photographs allow me to refer to the patient’s standing appearance while she is supine, and I can more accurately address her topography during the operation. This has been the most important single tool for me to obtain predictable results with fat grafting to the body.
Related posts:
 Chapter 46 AESTHETIC LIPOSCULPTING AND FAT GRAFTING FOR THE BUTTOCK AND TORSO
Chapter 46 AESTHETIC LIPOSCULPTING AND FAT GRAFTING FOR THE BUTTOCK AND TORSO
 Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
Chapter 7 AUTOMATED SYSTEMS FOR PROCESSING THE STROMAL VASCULAR FRACTION AND CALCULATING THE NUMBER OF STEM CELLS
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 48 LOWER EXTREMITY RECONSTRUCTION
Chapter 48 LOWER EXTREMITY RECONSTRUCTION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


