Chapter 41 RECONSTRUCTION OF BREAST DEFORMITIES
Breast malformations are uncommon deformities that are revealed during puberty and that carry negative psychological and physical impact for the individual. The clinical picture is variably complex: from simple asymmetries in volume, a physiologic difference between the breasts, to intricate frameworks with hypoplasia or aplasia of ribs and muscles. 1 A certain degree of asymmetry in the breasts is considered normal and acceptable if it is limited to a slight difference in volume; it is more difficult to accept an evident disproportion in volume, shape, or areolar contour. Different degrees of severity in asymmetry, or tuberous breast or Poland syndrome may be present. This is especially difficult for young women, often causing them discomfort and embarrassment and potentially compromising their social relations. A surgical approach is typically postponed until after complete development of the breast. However, sometimes surgery is best performed at an earlier age because of the patient’s emotional distress or when a long or staged reconstructive procedure is required.
Material and Methods
PREOPERATIVE EXAMINATION
The introduction of fat grafting to the breast has significantly changed our approach to treating breast deformities. 2 An implant-free surgical approach is very desirable, primarily in young women. Fat grafting, with its regenerative potential, represents the best option to obtain a natural, soft breast with long-lasting contours.
In the first consultation, after history-taking and a thorough physical examination, the surgeon must discuss the proposed procedure with the patient, explaining her morphologic anomalies, their degree of severity, the complexity of the required treatment, and any limitations of the procedure toward achieving her desired result. The potential complications, including swelling, bruising, ecchymosis, fat resorption, and pain in the donor and recipient sites, must also be addressed. It is essential to understand the patient’s psychological attitude and expectations so that she will be satisfied with the result.
Complete assessment begins with a careful physical examination. The breasts’ shape, volume, skin, and nipple-areola complex are evaluated. Bilateral differences in contour and volume are documented, photographed, and discussed with the patient. This will help the surgeon to estimate the amount of lipoaspirate that must be harvested to produce adequate volume for fat grafting to the breast. The thickness, elasticity, color, and texture of the skin should be carefully evaluated, and the presence of stretch marks should be noted. The breast parenchyma is assessed for texture, shape, and distribution in all four quadrants.
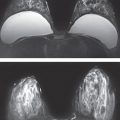
The presence of giant fibroadenomas or cancer, which may be misdiagnosed in the presence of breast asymmetry, should be assessed. Breast ultrasonography, mammography, and MRI are also essential to clarify volume and fatty or glandular breast structures and any indications of the presence of cancer.
Chest radiographs and CT scans are useful in patients with skeletal diseases or complex malformations. Abdominal ultrasonography is useful to exclude the kidney diseases that are frequently related to severe breast malformation.
Accurate photographs are essential to document the patient’s preoperative and postoperative appearance. Photographs are taken with the patient standing with her arms loose at the sides in frontal, oblique, and lateral views. These photographs help the surgeon to establish the reconstructive plan, document the changes, and confirm the results obtained after surgery and at each follow-up visit.
SURGICAL TECHNIQUE
Preoperative Planning
One month before each surgical session, the BRAVA System, an external expansion device (see Chapter 42), should be applied on the patient’s thoracic wall for at least 8 hours a day, usually during the night. The suction effect of the external expansion device serves to enlarge the breast’s fat grafting recipient site. This allows a larger amount of lipoaspirate to be injected at each session, resulting in the need for fewer procedures. 3 – 7
As the negative pressure expands the skin envelope, it also improves skin softness and increases the grade of ptosis in the treated breast. Thus the need for contralateral breast reshaping, mastopexy, or breast reduction can be avoided or reduced.
The BRAVA System should again be used as soon as possible after fat grafting, when the symptoms of bruising, pain, or ecchymosis have resolved, because it stimulates the proliferation of the adipose-derived stem cells (ADSCs), increasing the final volume of the breast. 8
Harvest of Lipoaspirate
The lipoaspirate is harvested while the patient is deeply sedated. An antibiotic solution is administered 30 minutes before the procedure begins. The donor areas in younger patients are primarily the flanks and trochanteric regions. The donor areas are infiltrated with a Klein solution: 500 ml of saline solution with 20 ml of lidocaine 0.5% and 1:400,000 epinephrine. 9 , 10
Fat is harvested with a multihole blunt cannula, 3 mm in diameter, connected to a 50 cc Luer-Lok syringe. The harvested fat parcels have smaller dimensions, thus enhancing the lipoaspirate distribution and take.
When sufficient fat has been harvested, the cannula is removed from the syringe and replaced with a plug. The syringes are placed in a bowl and left for decantation as long as necessary, usually not more than 20 minutes.
Purification
The lipoaspirate separates into three layers, the lower containing fluids, the middle containing the viable fat, and the upper containing oil from ruptured adipose cells. The oil and fluids are discarded, and the remaining purified lipoaspirate is transferred to 3 cc syringes for grafting. 6
Fat Distribution
Two main issues should be considered when performing fat distribution: the total amount of fat to be grafted and the homogeneity of the deposition.
The amount of fat grafted is patient specific. The fat is distributed in different planes—subpectoralis, subglandular, and subcutaneous—but should never be injected directly into the mammary gland. It is important to avoid applying too much pressure when injecting, while drawing back the cannula to minimize any risk of arterial or venous embolization. The ribbon of fat is placed as the syringe is withdrawn, not as it enters the tunnel. The stiffness of the subcutaneous tissue and the skin retraction are crucial factors and should be avoided to preserve some elasticity and softness of the breast tissues. 5 , 6
Homogeneity of the lipoaspirate distribution in the different layers maximizes its contact with the hosting tissue and increases the quality of the final results. 5 , 11 Injection of bulky quantities of fat results in fat necrosis, oil cysts, and macrocalcifications.
Results
The surgical approach to the correction of breast deformities must follow a precise sequential pattern. The surgical steps that we have developed over many years of clinical experience are as follows:
Fat grafting into the submammary crease
Rigottomies to lower the fold
Fat grafting in multiple layers
Filling and release of all quadrants with fat graft and rigottomies
Use of the BRAVA System
Each step must be executed in this order to allow for effective breast filling and shaping. This protocol is universal and can be applied to every patient, as demonstrated in the following clinical cases. Obviously, according to the needs of the specific patient some surgical steps will require more effort than others.
MODERATE BREAST ASYMMETRY
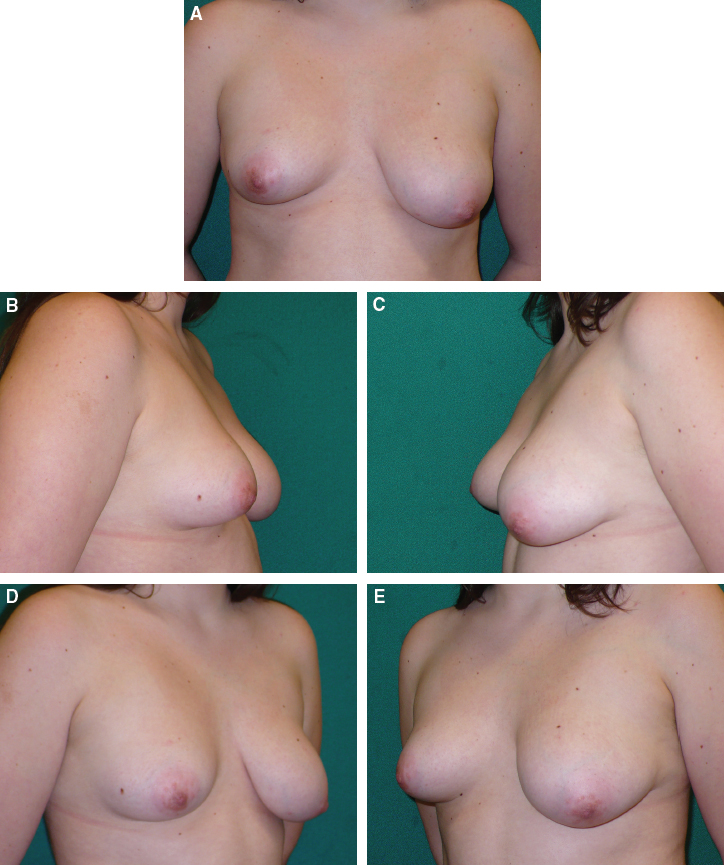
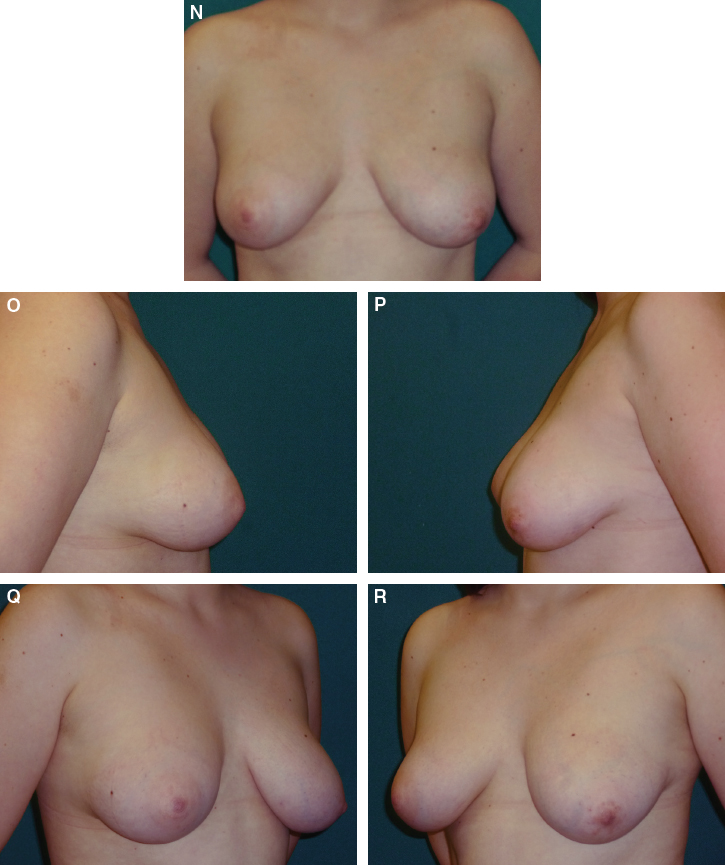
This 20-year-old patient had moderate breast asymmetry and requested fat grafting to correct this but did not want a mastopexy of the contralateral breast. The right breast was hypotrophic, and the left breast was ptotic, with the nipple-areola complex pointing downward. The skin was soft and elastic. Her breast footprints were symmetrical, with parallel inframammary folds.
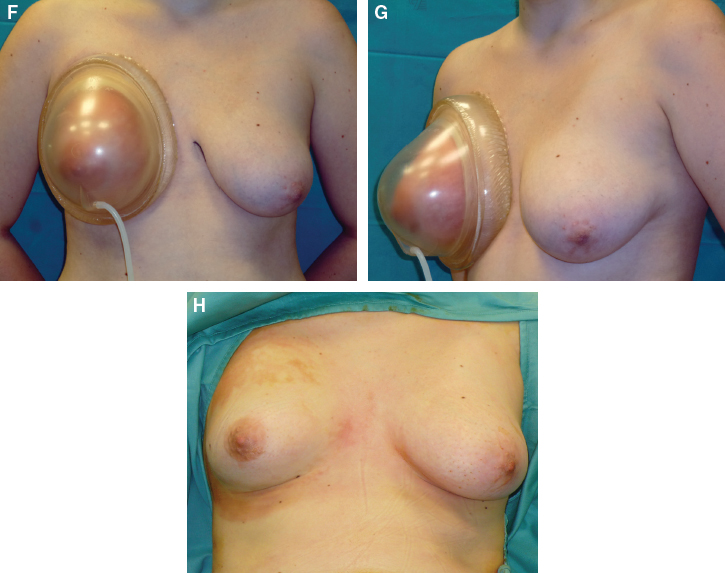
It was necessary to increase the volume and ptosis of the right breast. For the left breast, the plan was to reduce the breast ptosis. The patient wore the BRAVA device preoperatively and postoperatively only on the right breast for 8 hours a day, and it was removed immediately before surgery. In the left breast we injected a small amount of fat, about 30 to 40 cc, along the entire inframammary fold. To reduce the breast ptosis on the left, we had to reposition the fold at a lower level to increase the distance between the areolar edge and the inframammary fold.
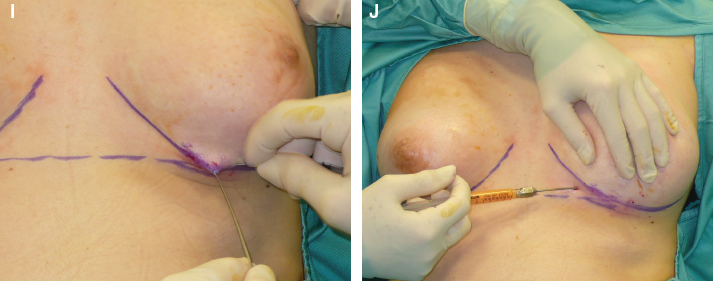
We performed rigottomies, a simple, noninvasive, and very effective approach. With a skin hook to keep the skin under tension, a 14-gauge needle is used to detach the entire inframammary fold from its original position. Debridement is carried out until the fold reaches the desired new position.
We injected some fat along the entire fold to prevent any retraction, thus stabilizing the result. This produced a left breast that was less ptotic, with a more natural appearance.
For the right breast, the operative plan was to increase both volume and ptosis of the breast. The right fold was symmetrical with the contralateral fold, so there was no need to reshape or reposition it.
To increase volume through fat grafting, the fatty tissue should be injected in different planes of the breast using a type II Coleman cannula. A very small amount of fat should be placed with each pass, using many passes, starting from the deepest layer, the infrapectoralis plane. It is safer to start fat grafting at the lateral quadrants, because it is easier to reach the correct plane. The procedure should be performed slowly and carefully to avoid damaging the underlying intercostal muscles or the pleura and to prevent serious complications, such as hematomas or pneumothorax.
The total amount of injected fat should be 60 to 80 cc. This procedure can improve the projection of the breast.
The retroglandular plane is injected next, again placing the parcels of fatty tissue in many tunnels and grafting a very small amount of fat with each pass. Different entrance points should be used to obtain a more homogeneous distribution of the fat. Injection of a bolus of fat must be avoided; that would lead to fat resorption and to oil cyst formation.
Next fat is injected in the subcutaneous plane. The lipoaspirate must be placed between the skin and the gland, all over the entire breast. This increases the softness of the breast and improves the breast contour. Fat should never be injected directly into the mammary gland.

Fat grafting was performed mainly at the level of the lower pole with blunt cannulas to increase breast volume. The pliability of the skin must be maintained to produce a natural feel and appearance to the breast.
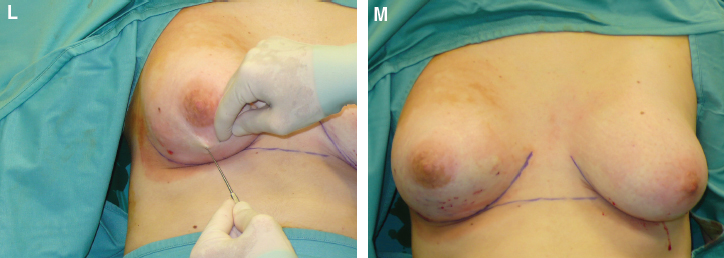
Rigottomies were performed at the entire surface of the lower pole to release the breast skin and produce ptosis to match the contralateral breast. The result at the end of the first fat grafting session is shown.
The patient underwent a second fat grafting procedure. The total amount of fat grafted was 530 cc (250 cc and 280 cc), and the reconstructive procedure was completed within 6 months. At 2-year follow-up, the breasts have good volume, symmetry, and equal degrees of ptosis.
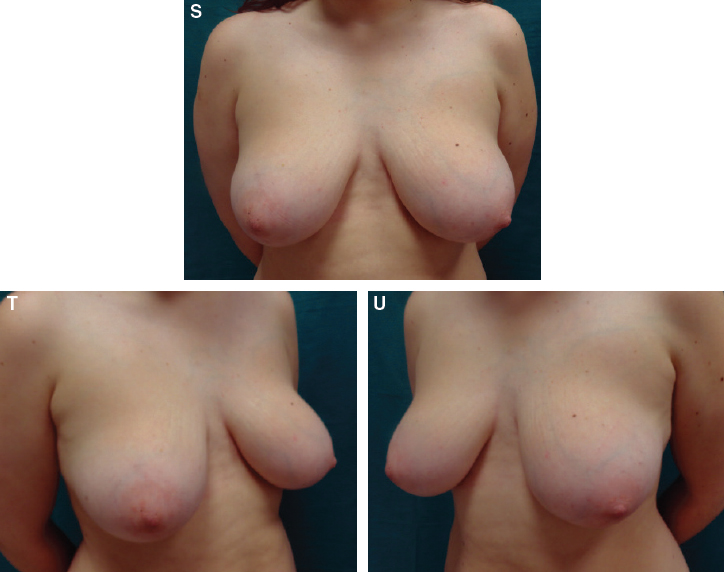
At the 4½-year follow-up visit, it was evident that the patient had gained a significant amount of weight. Both breasts increased in size proportionally, maintaining and improving the symmetry. The increase of breast volume is associated with an increase in the degree of bilateral ptosis.
Related posts:
 Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
Chapter 39 ONCOLOGIC RISKS OF FAT GRAFTING OF THE BREAST
 Chapter 40 LIPOMODELING FOR CONGENITAL BREAST DEFORMITIES: TUBEROUS BREASTS, POLAND SYNDROME, AND ASYMMETRY
Chapter 40 LIPOMODELING FOR CONGENITAL BREAST DEFORMITIES: TUBEROUS BREASTS, POLAND SYNDROME, AND ASYMMETRY
 Chapter 42 FAT GRAFTING FOR BREAST RECONSTRUCTION WITH EXTERNAL VACUUM EXPANSION
Chapter 42 FAT GRAFTING FOR BREAST RECONSTRUCTION WITH EXTERNAL VACUUM EXPANSION
 Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
Chapter 18 SCAR REMODELING WITH FAT GRAFTING AFTER BURN INJURY
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
 Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Chapter 45 IATROGENIC LIPOSUCTION DEFORMITIES
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


