CHAPTER 19 Sentinel Lymph Node Biopsy Outcomes
KEY POINTS
Sentinel lymph node biopsy (SLNB) is an oncologically safe procedure to identify the primary lymph node to which a solid tumor, such as a melanoma, breast cancer, or gynecologic cancer, is likely to drain.
Compared with nodal observation alone, SLNB increases overall and disease-free survival in patients with intermediate-thickness tumors.
The incidence of lymphedema has been reduced but not eliminated by the use of the SLNB technique.
The incidence of lymphedema after SLNB ranges from 4% to 9% in the three tumor types (melanoma, breast cancer, and gynecologic cancer) discussed in this chapter.
Patient-reported quality of life is affected less by SLNB than by total lymphadenectomy.
The use of the sentinel lymph node biopsy (SLNB) has changed the landscape for the surgical treatment of many types of solid tumors, including melanomas and breast cancer. This minimally invasive procedure identifies and resects sentinel lymph nodes (SLNs) for the pathologic staging of lymph node basins in patients at risk for nodal metastases and can be used to avoid the morbidity associated with a complete lymphadenectomy in patients with pathologically confirmed negative SLNs.
This chapter outlines the technique for performing a SLNB and highlights recent literature findings related to the efficacy of the procedure in different types of cancers. Finally, there is a discussion of the impact of SLNB on lymphedema and quality of life (QOL) outcomes related to the use of this technique.
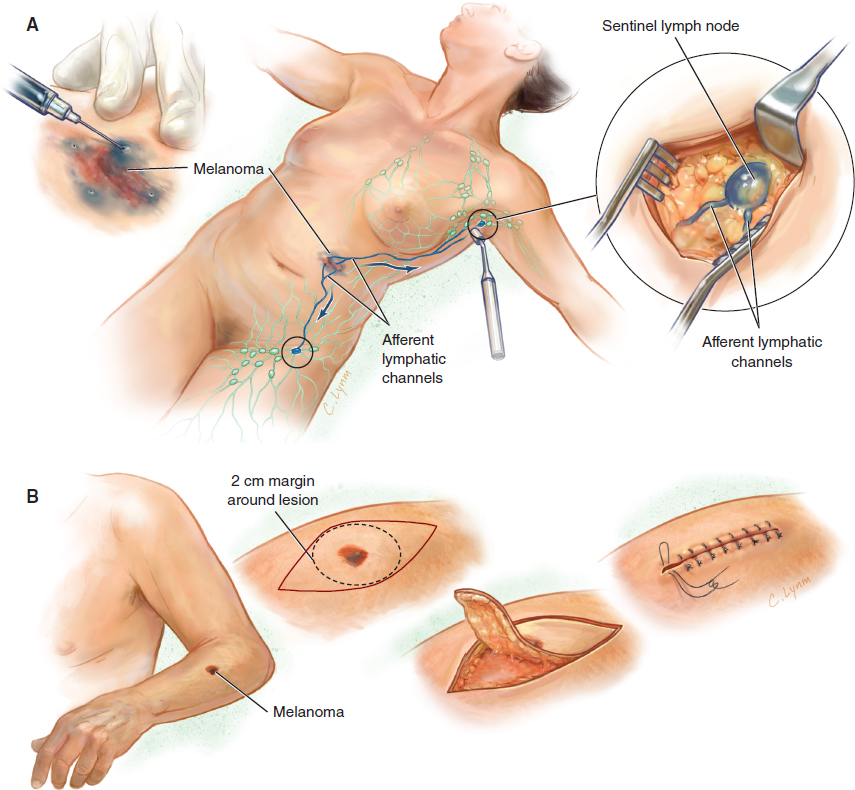
Gould et al 1 first described the concept of SLNB in 1960 after an incidental finding of a lymph node at the junction of the anterior and posterior facial veins during a total parotidectomy. After node removal and identification of metastatic tumor cells, a complete cervical lymph node dissection was performed. In 1977 Cabanas 2 published an article on SLNB at the time of surgical resection for penile cancer in which lymphatic imaging was used to identify the SLN. The SLN was then excised for immediate evaluation; on identification of tumor cells in the SLN, a total lymph node dissection was done. At about this time, Morton et al 3 investigated the various techniques of SLN identification—first in a feline model and subsequently in patients—by the intraoperative injection of isosulfan blue dye adjacent to primary melanoma sites to identify SLNs in the regional nodal basin 3 (Fig. 19-1).
In the early 1990s, SLNB was adopted for the pathologic staging of regional lymph nodes in patients with breast cancer. In 1996 a prospective trial of patients with invasive breast cancer who underwent SLNB before a completion axillary lymph node dissection (ALND) and segmental mastectomy or mastectomy within a single surgical procedure was reported. 4 In this trial the SLN was identified in 92% of patients, and a positive SLN was identified before ALND in all patients with positive nodal disease. Albertini et al 4 reported that this technique reduced surgical morbidity. This technique also gave pathologists the opportunity for an in-depth evaluation of fewer lymph nodes to more accurately identify micrometastatic disease.
SLNB has also been applied to gynecologic cancers. This procedure was initially piloted for the treatment of squamous cell carcinoma of the vulva. 5 In a prospective study of women undergoing routine lymphadenectomy, surgeons identified and excised the SLNs with preoperative lymphoscintigraphy and intraoperative blue dye and subsequently performed a completion inguinofemoral lymph node dissection (ILND). Metastatic nodal disease was pathologically confirmed in almost half of the patients, each of whom had a positive SLN. 5
Breast and cervical cancers are the first and fourth most commonly diagnosed cancers in women worldwide; an estimated 1,676,633 new cases of breast cancer and 1,085,948 new cases of cervical cancer are diagnosed annually. 6 Melanoma is one of only a handful of cancers with an increasing annual incidence worldwide; an estimated 232,130 cases were diagnosed worldwide in 2012. 6 With an overall estimated incidence of lymphedema of 6% for breast cancer, 4% for melanoma, and 9% for gynecologic cancers after SLNB, we estimate that 207,617 people will be diagnosed annually worldwide with lymphedema after SLNB, and many more are at a significant lifetime risk. 7
Surgical Technique
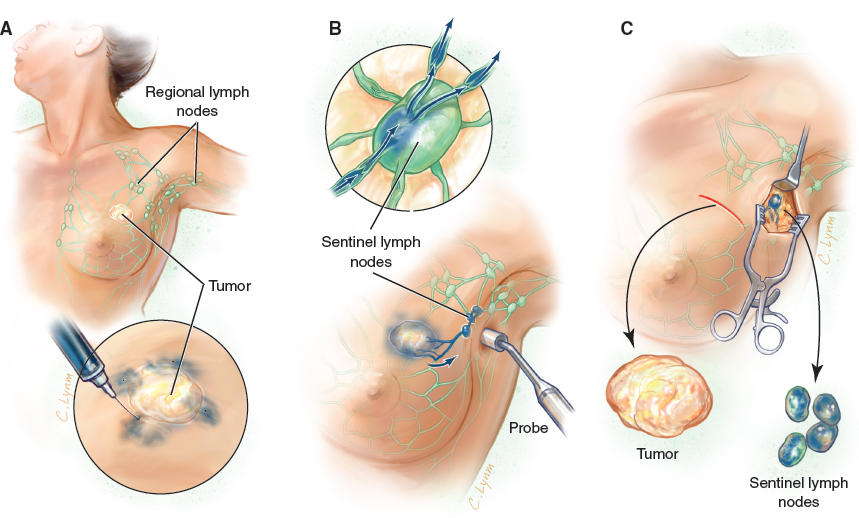
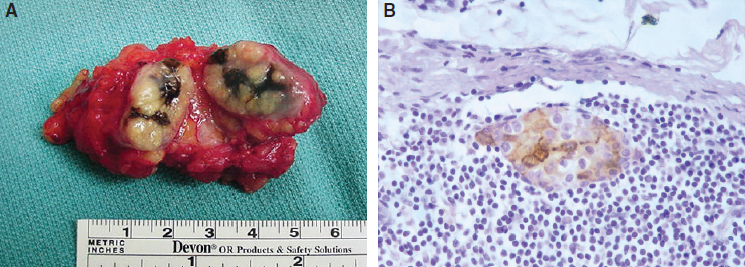
The current standard technique for SLNB is as follows. To facilitate the accurate identification of SLNs, blue dye is injected at the site of the primary tumor, turning the SLNs blue. Radioisotopes can also be injected at the primary tumor to guide surgeons to SLNs harboring radioactivity, regardless of color uptake (Fig. 19-2). Current techniques for SLNB most commonly use technetium-99m (99mTc)-sulfur colloid (in the United States), 99mTc-nanocolloid (widely used in Europe), or 99mTc-antimony trisulfide colloid (used in Australia) as a radiopharmaceutical agent. 8 After the blue dye and radioactive isotope are injected, the surgeon uses a gamma-detecting probe to help localize sites of high radioactivity in the lymph node basin (see Fig. 19-2). An incision is made at a regional nodal basin site that has significant radioactivity, and the nodal tissue is dissected to identify blue and/or radioactive lymph nodes. The SLN or SLNs are excised from the remaining contents of the nodal basin and undergo pathologic assessment (Fig. 19-3).
The accuracy and sensitivity of SLNB have been shown in most cancer types in which the procedure is part of the current treatment recommendations. When SLNB was done according to the standard treatment guidelines, the accuracy was 97%, sensitivity was 91%, specificity was 100%, and negative-predictive value was 95% in breast cancer. 9 Similar numbers have been found in melanoma studies. A systematic review and meta-analysis by Meads et al 10 evaluating SLNB in vulvar cancer found that the accuracy of the procedure (when done with both a blue dye and radioactive tracer) was 98%, sensitivity was 95%, and negative-predictive value was 98%.
Impact on Outcomes
LONG-TERM SURVIVAL OUTCOMES
The first evaluation of the impact of SLNB on survival was conducted in a multiinstitutional, randomized, controlled trial, the Multicenter Selective Lymphadenectomy Trial (MSLT-1), led by Morton. 11 In this trial patients with melanoma were randomly assigned to receive a wide local excision and either SLNB or nodal observation only. Ten-year follow-up data on more than 1500 patients were available for the final analysis, which was published in 2014. 12 Statistically, the 10-year melanoma-specific survival rates were significantly higher in patients who received SLNB (81.4% ± 1.5%) than in those who had nodal observation only (78.3% ± 2.0%). In light of these findings, the National Comprehensive Cancer Network guidelines have included recommendations for the pathologic staging of melanoma in patients with primary tumors that are thicker than 0.75 mm or a primary tumor of any thickness that is ulcerated or has at least one or more mitotic figures per high-power field. 13
LYMPHEDEMA OUTCOMES
Lymphedema has long been recognized as a potential morbidity after a complete lymph node dissection for many solid tumors. 7 In a systematic review of non–breast cancer lymphedema, Cormier et al 7 identified 47 studies across five categories of malignancies (melanoma, gynecologic cancer, genitourinary cancer, head and neck cancer, and sarcoma) that reported incidences of lymphedema ranging from 4% to 40% after complete lymph node dissection.
Recently SLNB has also been recognized as a risk factor for lymphedema; however, the risk is significantly less than that of complete lymph node dissection. Tables 19-1, 19-2, and 19-3 summarize the peer-reviewed publications (2000 to 2014) reporting the incidence of lymphedema after SLNB for breast cancer, melanoma, and gynecologic malignancies. There is significant heterogeneity in the measurement techniques used to quantify lymphedema, which included water displacement, perometry, and limb circumference measurement.
Melanoma
Six studies that included patients with melanoma undergoing SLNB and reported data on lymphedema outcomes were identified. The weighted pooled incidence of lymphedema was 4% (range 0.6% to 15%) (Table 19-1). In a systematic review of lymphedema in non–breast cancer solid tumors, Cormier et al 7 found that the pooled lymphedema incidence was 18% after ILND and 3% after ALND. In a prospective study designed to assess lymphedema after SLNB or complete lymph node dissection (axillary or inguinofemoral) for the pathologic assessment and treatment of cutaneous melanoma, Hyngstrom et al 14 used perometry to measure the limb circumference of patients with lymphedema before and after surgical intervention (lymphedema was defined as a 10% increase in limb volume from baseline) and assessed subjective, patientreported symptoms of lymphedema with a validated instrument, the 19-item Lymphedema and Melanoma Questionnaire. Twelve months after surgery, 15% of patients who underwent SLNB and 30% of those who underwent lymph node dissections had objectively measured lymphedema. The highest incidence of lymphedema was in patients who had an ILND, 46% of whom had objectively measured lymphedema 12 months after surgery. 14
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


