Chapter 15 CRYOPRESERVATION OF ADIPOSE TISSUE FOR FAT GRAFTING
Currently, lipoaspirate can only be used for immediate structural fat grafting during the same procedure in which liposuction is performed; therefore excess harvested, purified lipoaspirate from the procedure is usually discarded. Both plastic surgeons and patients have valid reasons to want to preserve the harvested adipose tissue long term, if an optimal technique were available, for use in future applications to that patient. However, simple freezing of fat grafts with liquid nitrogen should not be considered as a standard method for long-term preservation of fat grafts, because this leads to poorly maintained viability of the purified lipoaspirate and a higher degree of resorption after it is transplanted. Without adding cryoprotective agents to adipose tissue before cryopreservation, the results have clearly been poor, based on our in vitro study, and this was again confirmed by the findings from our in vivo study. 1 – 3 Undoubtedly, the development of a practical and optimal cryopreservation technique will benefit many patients who desire soft tissue augmentation with their own fat for either cosmetic or reconstructive reasons.
With the current strategy proposed for the use of processed adipose tissue cells for cell-based tissue engineering and transplantation, the harvested lipoaspirate would be processed immediately for processed cells after they are collected by conventional liposuction, and then these cells would be stored by means of one of the tissue banking techniques (cryopreservation). 4 , 5 One of our studies demonstrated that after cryopreservation with our preferred technique, human lipoaspirate may be a reliable source of adult human processed lipoaspirate cells, because they could be processed later in sufficient quantities for fat grafting. 6
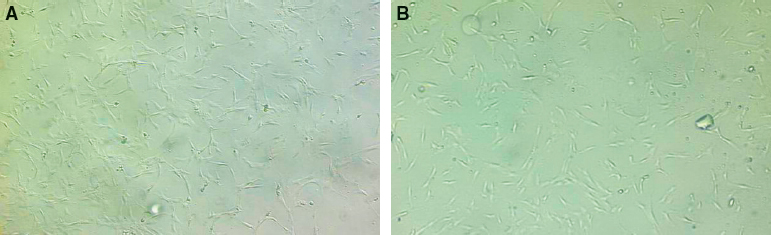
Flat, spindle-shaped, processed lipoaspirate (PLA) cells after a 2-week culture from the fresh control group are shown (A) and from the cryopreservation group (B). Phase-contrast microscopy was used with an original magnification of 100×. Both PLA cell samples appear to have normal morphology and may be used for cell-based therapy in the future.
Modern Techniques in Cryopreservation
The modern technique of cryopreservation permits the long-term storage of living cells and tissues that may have many potential clinical applications such as blood transfusion, bone marrow transplantation, in vitro fertilization, vascular grafts, bone grafts, and skin grafts. 1 The major steps of the cryopreservation process can be summarized as follows: (1) add cryoprotective agents to cells/tissues before cooling, (2) cool the cells/tissues in a controlled rate toward a low temperature at which the cells/tissues are stored, (3) warm the cells/tissues, and (4) remove the cryoprotective agents from the cells/tissues after thawing. 7 The optimal cooling rate for cell survival should be slow enough to avoid intracellular ice formation but fast enough to minimize cell damage.
The freezing behavior of the cells can be modified by the addition of cryoprotective agents, which affect the rates of water transport, nucleation, and crystal growth. Cells that have survived cooling still face the challenges of thawing, which can exert effects on survival comparable to those of cooling. Also, knowledge of the cell permeability to water and cryoprotective agents allows one to predict minimal and maximal cell volume excursion during the addition and removal of cryoprotective agents in the cells to provide a quantitatively optimal approach toward avoiding osmotic damage.
Dimethyl sulfoxide (DMSO), a permeable agent, has been widely used as an effective cryoprotective agent (CPA) in the cryopreservation of living cells or tissues. 7 , 8 The concentration of DMSO, when used alone as a CPA, is usually 10%. Because this agent is tissue toxic at normal body temperature, it should be removed from the previously cryopreserved cells or tissues after thawing. In our previous study, we attempted to lower the concentration of DMSO used in cryopreservation of adipose tissue by adding another nontissue toxic cryoprotective agent, such as trehalose. As a CPA, trehalose can dehydrate cells and thus reduce the amount of water present before freezing. It can also stabilize cellular membranes and proteins during freezing and drying. Combining trehalose, a nonpermeable cryoprotective agent, with DMSO, a permeable cryoprotective agent, may work synergistically to protect adipose tissue during cryopreservation. 9 Therefore the concentration of DMSO can theoretically be reduced when it is used in combination with trehalose. The combined use of both DMSO and trehalose as cryoprotective agents may be valuable to achieve optimal cryopreservation of adipose tissues or other types of tissues.
Previous Studies in Cryopreservation of Fat Grafts
A simple freezing technique has been recently used by a number of investigators to explore the possibility of long-term storage of fat grafts. In one study, fat grafts were frozen in liquid nitrogen and stored at –195.8° C for up to 8 days. The results demonstrated that the frozen fat grafts showed remarkable maintenance of mitochondrial metabolic activity. 10 However, a separate study by others indicated that after simple freezing, up to 92.7% of metabolic activity of fat grafts was lost, but the addition of a CPA led to preservation of up to 54% of the baseline activity. 11 The authors indicated that the widely used practice of simple freezing in a freezer leads to nonviable tissue and cell survival can be improved by the addition of a CPA. In another study, fat grafts were simply frozen in liquid nitrogen and stored at –35° C for 6 months. Interestingly, these authors found that the viability and histologic characteristics of fat grafts frozen in liquid nitrogen were similar to those of fresh grafts. 12 However, their finding has been questioned by other investigators, who have found that to achieve optimal cryopreservation of adipose tissue, it would be necessary to add a CPA before freezing and fat grafts mixed with a CPA should also undergo controlled freezing and thawing during cryopreservation. 1 – 3 , 13 , 14
In our laboratory, a preliminary study was conducted earlier to evaluate the effect and role of temperature alone for storage of adipose tissue. In these studies, the viability of lipoaspirate that underwent “low” temperature banking was assessed by a glycerol-3-phosphate dehydrogenase (G3PDH) assay at both 4° C and –20° C. The G3PDH assay was chosen in our study to assess cellular function of adipose tissue because it is relatively simple and the enzyme is adipose specific. The assay measures the level of G3PDH within the cytoplasm of adipocytes. The higher level of the enzyme represents a better cellular function of adipose tissue. 15
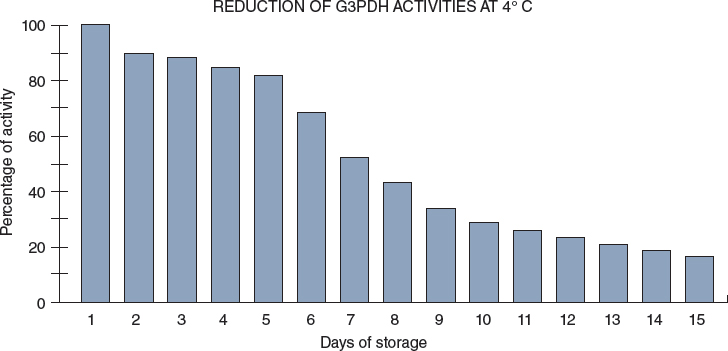
After 2 weeks of storage, the viability of adipose aspirates decreased by about 80% at 4° C.
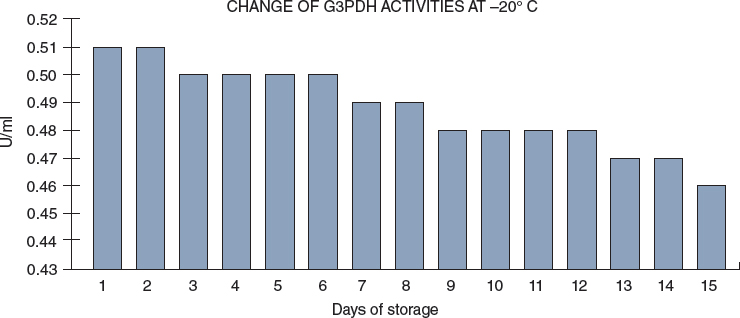
By contrast, the viability of lipoaspirate decreased by only about 5% at –20° C in 2 weeks. Furthermore, a series of experiments was performed initially with different types and concentrations of cryoprotective agents, and their different combinations to determine what would be the best CPA that can be used especially for adipose tissues.
Although a few studies showed encouraging preliminary results for cryopreservation of autologous fat grafts for possible future application, the technique described in the study can only be used for a short-term preservation (a few days or weeks) and may not be optimal due to uncontrolled cooling/warming process and the lack of use of a cryoprotective agent. With application of modern cryopreservation techniques, a better long-term preservation of adipose tissues can possibly be performed. Such a method will likely allow fat grafts to be stored for months or years (below –85° C) or for more than 10 years (at –196° C in liquid nitrogen).
We conducted a preliminary study with the use of modern cryopreservation technique for cryopreservation of lipoaspirates. Our initial results are quite encouraging and proper cryoprotective agents and their optimal concentration or combination can be selected.
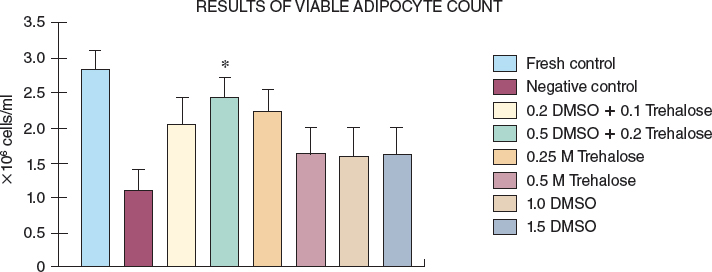
Results of the viable adipocyte count in different cryoprotective agent–treated groups are shown: *p >0.00625 versus all other CPA groups except the 0.25 molar (M) trehalose group; p = 0.083 (NS) versus the 0.25 M trehalose group; p = 0.014 (NS) versus the fresh lipoaspirate. It becomes clear that a combination of 0.5 M DMSO and 0.2 M trehalose can be the best selection for cryoprotective agents that should be used during cryopreservation of adipose tissue. 3 In addition, trehalose alone may also be used for cryoprotection of adipose tissue. 16 A number of freezing and thawing protocols were also evaluated for adipose tissue during the preliminary studies.
Again in our laboratory, we conducted additional studies to determine whether trehalose alone can be used as an effective cryoprotective agent. We calculated the viable adipocyte counts in different concentrations of trehalose groups. The highest viable adipocyte count was found in the trehalose group with a concentration of 0.35 mol/L, p>0.05 versus the fresh control group and p>0.001 versus all other trehalose groups. Trehalose, as a CPA with a concentration of 0.35 mol/L, appears to provide optimal protection of lipoaspirate during the cryopreservation in vitro and in vivo with the same freezing and thawing protocol developed in our laboratory. 17 Such protection is found to be similar to that provided by a combination of 0.5 M DSMO and 0.2 M trehalose as CPAs. 18
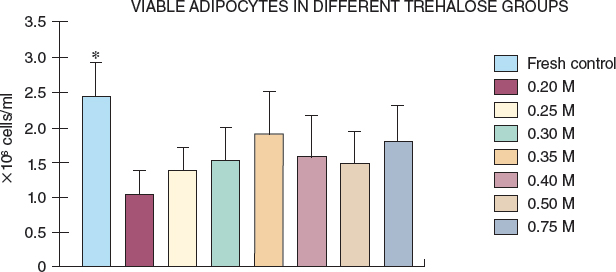
Viable adipocyte counts in different concentrations of trehalose groups. The highest viable adipocyte count was found in the trehalose group with a concentration of 0.35 mol/L, p>0.05 versus the fresh control group and p>0.001 versus all other trehalose groups.
Related posts:
 Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
 Chapter 12 THE PHYSIOLOGY OF INJURED, OBESE, GRAFTED, AND DYING FAT
Chapter 12 THE PHYSIOLOGY OF INJURED, OBESE, GRAFTED, AND DYING FAT
 Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
 Chapter 14 PLATELET-RICH PLASMA AND FAT GRAFTING
Chapter 14 PLATELET-RICH PLASMA AND FAT GRAFTING
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


