Chapter 14 PLATELET-RICH PLASMA AND FAT GRAFTING
Breast reconstruction with autologous fat graft has become a commonly performed procedure in recent years. Many investigators have contributed to the development of the technique, adding the stromal vascular fraction (SVF), or growth factors, to the harvested fat. This technique has been applied for correction of breast defects and for repair of radiotherapy-based tissue damage after mastectomy, 1 breast augmentation, 2 postmastectomy breast reconstruction, 3 complications of breast implant surgery, 4 calvarial defects, 5 Crohn fistulas and complex perianal fistulas, 6 , 7 damaged skeletal muscle, 8 Parry-Romberg syndrome and facial lipoatrophy, 9 scarring, gluteal soft tissue defects, pectus excavatus, dermatofibrosis, 10 and vocal fold augmentation. 11
In Europe, and more recently in the United States, a trend has emerged in which autologous blood products are mixed with harvested fat for fat grafting to facilitate tissue regeneration and healing. We published the results of our study on the use of harvested fat combined with platelet-rich plasma (PRP) for improving fat volume in soft tissue defects and in breast reconstruction. We followed the lipostructure technique described by Coleman 12 , 13 ; our purpose was to determine the effects of combining the lipoaspirate with PRP 14 for the treatment of lower extremity chronic ulcers, 15 hemifacial atrophy, 9 and breast reconstruction. 16 , 17 We compared the results of grafting with this combination with those of a control group in whom only centrifuged fat was injected. Patient self-assessment of the outcomes was obtained as an additional parameter supporting the results of clinical assessment.
Platelet-Rich Plasma and Fat Grafting Preparation Based on Current Regulations
Our study was conducted with the informed consent of the patients and in the presence of a physician from the transfusion service, in accordance with the current Italian regulations. Briefly, the process of preparing PRP consists of four phases:
Blood collection
Centrifugation for platelet concentration
Induction of gelation (if the PRP is to be used in gel form)
Activation
In general, most systems, whether for large- or small-volume collection, do not concentrate the plasma proteins of the coagulation cascade. Therefore the set of rules must be shaped using products that maintain the quality standards of biopharmaceutical drugs. Accordingly, the regulations are linked to the related laws, which describe a complex pathway for authorization. Regulation No. 1394/2007 of the European Parliament for Advanced Therapies has defined bioprocess engineering products.
This definition excludes products that contain or are made exclusively of cells and nonvital human or animal tissues and that do not have pharmacologic, immunologic, or metabolic action. Included among the advanced therapy pharmaceutical products are those used for gene and somatic cell therapy (Directive 2001/83/[European Parliament] European Community, Annex I). 18 Cells and tissues are to be considered products of bioprocess engineering if they undergo “considerable manipulation.” The same regulation defines the difference between extensive and minimal manipulation and lists those that are considered relevant.
BLOOD COLLECTION
We prepared PRP using two methods:
From a small volume of blood (18 ml), using the Cascade-Selphyl-Esforax system (Aesthetic Factors, LLC), 9 , 14 , 15 with modifications
From a large volume of blood (60 to 120 ml), in accordance with the Platelet Rich Lipotransfert (PRL) system (Corios)
Briefly, blood was taken from a peripheral vein using sodium citrate as an anticoagulant.
CENTRIFUGATION FOR PLATELET CONCENTRATION
The traditional preparation of PRP consists of a slow centrifugation, which allows the platelets to remain suspended in the plasma, whereas the leukocytes and erythrocytes are displaced to the bottom of the tube.
In our current system for preparing platelet concentrations, we have used a wide variety of centrifuges. When PRP was prepared from a small volume of blood (18 ml) according to the method of the Cascade-Selphyl-Esforax system, with modifications, we centrifuged the blood at 1100 g for 10 minutes. When PRP was prepared from 60 ml of blood according to the PRL system, with modifications, using PRP alone (CPunT; Biomed Device) without the SVF cells, we centrifuged the sample at 1200 rpm for 10 minutes.
FAT GRAFT CENTRIFUGATION ACCORDING TO THE PLATELET RICH LIPOTRANSFERT SYSTEM
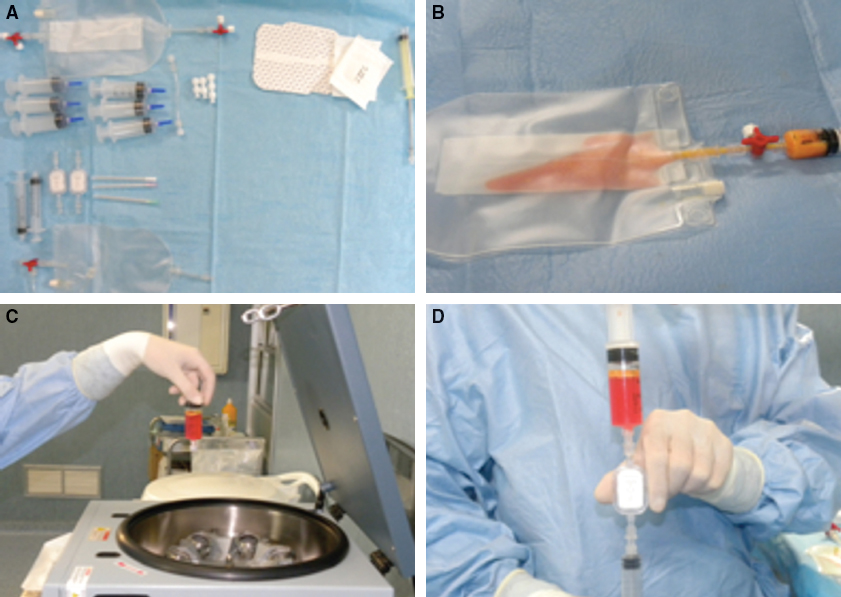
Before proceeding to the activation of PRP, with the patient under general anesthesia, we harvested fatty tissue from the abdominal region using some specific cannulas. To begin the PRL procedure, Fastkit materials were assembled for processing (A). In this instance, 80 cc of fat was subjected to automatic filtration (B). The fat harvested was centrifuged at 1700 rpm for 10 minutes (C), after which 40 cc of the suspension was extracted from the bag. The suspension was further filtered through a 120 µm filter, and 20 cc of the enhanced SVF (e-SVF) suspension was obtained (D). Subsequently the e-SVF suspension was added and mixed with the centrifuged fat graft. Using specific microcannulas for implantation, the e-SVF fat graft was transferred into 10 cc syringes. We mixed 0.2 cc of PRP with 1 cc of e-SVF centrifuged lipoaspirate and aseptically reinjected the mixture into the soft tissue defects.
Implantation
The recipient sites had been identified by thorough study of the corrections required. For facial soft tissue defects, enhanced fat graft was implanted in the zygomatic region, cheek, buccal rim, upper and lower eyelids, temporal area, and periorbital area. The fatty tissue was implanted at different levels in the small tunnels previously created by injecting the cannulas (1.5 mm in diameter) with accurate and controlled movements. Small quantities of fat were placed, one or two at a time, as the cannula was withdrawn, creating a large grid to facilitate a correct vascular contact and development around each fat cell.
For breast augmentation, enhanced harvested material was implanted mainly into three areas: the inferior breast rim, the superior and inferior regions of the areola, and the superolateral quadrant. After pretunneling, fatty tissue was implanted (average 280 cc total; range 80 to 400 cc average 120 cc for each breast) at different levels using a delivery cannula (1 or 2 mm in diameter) with precise, controlled movements. Several layers were laid down to increase the contact surface between the receiving tissue and the implant; this technique is of fundamental importance to allow each layer of deposited fat to survive by diffusion during the critical first few days necessary for growth of blood vessels to nourish the implant permanently. 1 , 2 , 5 , 11 The incisions were closed with 5-0 nylon sutures, and no compressive bandage was applied.
Results
PLATELET-RICH PLASMA AND INCREASES IN ADIPOSE TISSUE
In our series, PRP induced an increase of the number of adipose-derived stem cells (ADSCs) with no morphologic changes compared with the control group. The increase was statistically significant, by approximately fourfold, at 4 and 6 days, when cells were preconfluent (p <0.02). After 8 days, at confluency, there was a threefold increase of ADSC numbers in PRP cultures compared with the control group. Oil Red O staining revealed no significant difference in intracytoplasmic lipid accumulation between the PRP-treated and control ADSCs.
CLINICAL EVALUATION
Two methods for the clinical evaluation of outcomes were utilized: the team evaluation and the patient self-evaluation. 16 The team evaluation was based on clinical observation, using a scale of six values (excellent, good, discreet enough, poor, and inadequate). The patient self-evaluation used the same six values. The factors/variables that were taken into account were pigmentation, vascularization, pliability, thickness, itching, and pain.
The percentage of maintenance restored was clinically evaluated using two different criteria: subjective evaluation and objective evaluation. Subjective evaluation was based on the personal score of each patient, focused on the following parameters: (1) the presence of asymmetry, deformity, irregularity, dyschromia, dysesthesia, paresthesia, and pain, (2) results in the superolateral quadrant, inferolateral quadrant, superomedial quadrant, and inferomedial quadrant in breast reconstruction, (3) resorption of fat in one or more regions, (4) the time to stabilization of the transplanted fat, and (5) the need for retreatment. For each parameter, patients gave a yes or no (or positive or negative) response, and the percentage of maintenance restored was calculated as the mean of all calculated single percentages.
The objective evaluation was based on analysis of the preoperative and postoperative photos. The photos were of the same size, brightness, and contrast. According to the parameters listed above, the operator similarly calculated the percentage of restored material. Finally, the mean of patient and operator evaluations was calculated. 17 , 18
Related posts:
 Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
 Chapter 12 THE PHYSIOLOGY OF INJURED, OBESE, GRAFTED, AND DYING FAT
Chapter 12 THE PHYSIOLOGY OF INJURED, OBESE, GRAFTED, AND DYING FAT
 Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
 Chapter 15 CRYOPRESERVATION OF ADIPOSE TISSUE FOR FAT GRAFTING
Chapter 15 CRYOPRESERVATION OF ADIPOSE TISSUE FOR FAT GRAFTING
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


