CHAPTER 14 Facial Fat Grafting in Men
Summary
Adherence to these fat grafting principles encourages longevity, promotes stability, and effectively integrates the fatty tissue into the host tissues of male patients. Fat grafted in this fashion creates a definitive structural change that is integrated and that can positively affect the tissues into which it is placed. The philosophy of the Coleman fat grafting technique remains fundamentally unchanged since its original publication in 1994. The Coleman technique continues to be the world’s gold standard of fat grafting after three decades of clinical application. The following is an overview of the basic principles of the Coleman technique, from harvesting through placement.
Introduction
Fat is considered an ideal filler, and at the same time it plays a key role in tissue regeneration. For men, the applications are numerous. However, the field of autologous fat grafting has a varied history.
The minimally invasive character of the fat grafting procedure is the result of a long evolution of ideas, first developed at the end of the 19th century (1893) by Gustav Neuber (1850–1932). 1 Neuber transferred adipose tissue en bloc from the arm to the orbit to correct depressed and unpleasant scars sequelae of osteomyelitis. During the first decade of the 20th century, Eugene Holländer (1867–1932), 2 proposed the injection of a cocktail of human and ram fat into specific areas to be treated.
Surgeons confronted with fat grafting empirically noted two aspects of the procedure. The first, is the healing potential of fat. For example, the power of the adipose-derived stem cells may explain why fat placed into the wounds of the facially disfigured soldiers from World War I is effective for accelerating the healing process. 3 , 4 On the other hand, the reabsorption rate was considered a frustrating drawback. Lyndon Peer (1898–1977) demonstrated in the 1950s that about 50% of fat cells rupture and die after transplantation and that they are replaced by fibrous tissue. 5 For this reason and for the unpredictable results obtained, the technique was abandoned.
The recent surge in popularity of autologous fat grafting has made this into a challenging new field of research and clinical applications in both aesthetic and reconstructive plastic surgery. It has completely revolutionized our specialty and replaced numerous complicated operations with a minimally invasive procedure. However, there are numerous unanswered questions in fat grafting, especially those that surround best practices for harvesting, processing, placement, and recipient site preparation. 6 Techniques have been considerably refined over the years, but they have not yet been standardized. We still do not know the ideal method for each of the steps of fat transfer. This chapter will address some important techniques in relation to facial fat grafting in the male patient.
Patient Evaluation
Determine the specific amount of fat, and the levels of placement necessary to execute subtle contour changes in the face requires a well-developed strategy.
Before a plan can be developed, the surgeon must evaluate the patient’s lifestyle and social history, goals and expectations, prior aesthetic procedures, medical history, and physical appearance.
Have a precise plan. This is imperative because the Coleman fat grafting involves increments as small as 0.25 mm and rarely more than 3 or 4 mm.
Develop a rapport with the patient and encourage active patient participation in decision making.
If patients are interested in rejuvenation procedures, request that they bring photographs of themselves when they were young to help determine the degree of augmentation needed. By studying their old photographs, patients clarify their likes and dislikes and usually arrive for the first consultation with a much greater understanding of their own face and aesthetic preferences.
If patients are interested in enhancing their facial features or adjusting their facial proportions, ask them to bring in photographs of persons they think are attractive who have facial structures similar to theirs. These photographs give a better understanding of a patient’s aesthetic preferences.
During the initial consultation, focus on the patient’s lifestyle and social history, specific goals and expectations, history of previous aesthetic surgery procedures, medical history, and physical appearance. Take photographs that will be reviewed when the patient returns.
Obtain a complete history of a patient’s past aesthetic procedures that could influence the planned structural fat grafting. Because the presence of scars on the skin can influence the approach for placement of fat grafts, the history should include information about skin biopsies, punch biopsies, and so on.
Because the Coleman fat grafting is invariably an elective procedure, approach candidates with a poor general health status with caution.
The primary physician and anesthesiologist should confirm the patient’s ability to undergo the chosen type of anesthetic.
Address problems with bleeding, bruising, and unusual swelling after prior procedures to prepare the patient and surgeon for similar problems that might occur.
Give a list of medications to avoid to the patient at least 2 weeks before the planned procedure date 7 ( Table 14.1 ). Of particular importance is the effect of certain medications on platelet function.
Suggestions for Obtaining the Best Youthful Photographs
Ask for photographs in which the patient is not smiling, because smiling distorts the face, especially the cheeks, lower eyelids, and lips. However, photographs of the patient smiling can be useful for assessing the upper eyelids and forehead.
Request profiles as well as frontal views because profiles can provide the best information about the jawline and chin.
Remind patients to supply good-quality photographs that are in focus. Wedding photographs, expired passports, old yearbooks, and driver’s licenses are good sources. However, Instamatic photographs, Polaroid shots, and others may also be helpful.
Obtain a neurological history. This is essential. Fat infiltrated into the muscles of a patient who has recovered from a facial nerve injury or Bell’s palsy may act as a stent, inhibiting movement in the affected areas of the face.
Obtain any history of psychiatric problems and their current status. These may require special attention to prepare patients for the postoperative period.
Because smoking may impede the neovascularization of the grafts, and subsequent persistence of the grafted fat, actively discourage patient smoking before and after fat grafting.
Although the Coleman technique has resulted in successfully transplanted fat in several patients with autoimmune diseases (ulcerative colitis, rheumatoid arthritis, and systemic lupus erythematosus), there has been noted unusual postoperative problems in several patients with chronic fatigue syndrome, specifically prolonged swelling and pain in donor and recipient sites. Proceed with caution.
(Modified from SR Coleman, RF Mazzola, LLQ Pu. Fat Injection: From Filling to Regeneration. 2nd ed. New York, NY: Thieme; 2018.)
Supplements to Discontinue During The Fat Grafting Preoperative Period
Bilberry (Vaccinium myrtillus).
Cayenne (Capsicum annuum).
Dong Quai (Angelica sinensis).
Echinacea (Echinacea angustifolia).
Feverfew (Tanacetum parthenium).
Garlic (Allium sativum).
Ginger (Zingiber officinale).
Ginseng (Panax ginseng/Panax quinquefolium).
Hawthorn (Crataegus laevigata).
Kava kava (Piper methysticum).
Licorice root (Glycyrrhiza glabra).
Ma huang (Ephedra sinica).
Melatonin.
Red clover (Trifolium pratense).
St. John’s wort (Hypericum perforatum).
Valerian (Valeriana officinalis).
Vitamin E.
Yohimbe (Corynanthe yohimbe).
(Modified from SR Coleman. RF Mazzola, LLQ Pu. Fat Injection: From Filling to Regeneration. 2nd ed. New York, NY: Thieme; 2018.)
Anatomy
Related to Fat Harvesting
Males and females differ greatly in body fat distribution. Women generally have higher adiposity than men; in particular, men accumulate more fat in the central area (trunk and abdomen), and women accumulate more fat in the lower body (gluteal–femoral region). 8 In women, adipose tissue forming the mammary fat pad plays an important role in the development of the mammary gland and after puberty in the regulation of epithelial cell proliferation and function. In addition, women have a lower percentage of visceral adipose tissue than men do, even when they have a higher body mass index, total body fat, and abdominal subcutaneous adipose tissue values. 9
The reasons for this sexual dimorphism are not clear; much investigative attention is focused on sex steroid hormones. For instance, women with polycystic ovary syndrome, characterized by a hyperandrogenic state, are prone to central obesity, 10 whereas testosterone-treated men have less fat mass, with selective loss of central fat. 11 There are pronounced regional differences of the body in the regulation of regional fatty acid metabolism between men and women. 12
Kotani et al. 13 revealed a sex dimorphism in comparing regional adipose tissue distribution across age groups. In particular, they noted an increase of visceral white adipose tissue with age, mostly in men and postmenopausal women. These are important underlying sexual differences, because they are closely related to the incidence of cardiovascular diseases in men and women.
Related to the Aging Male Face
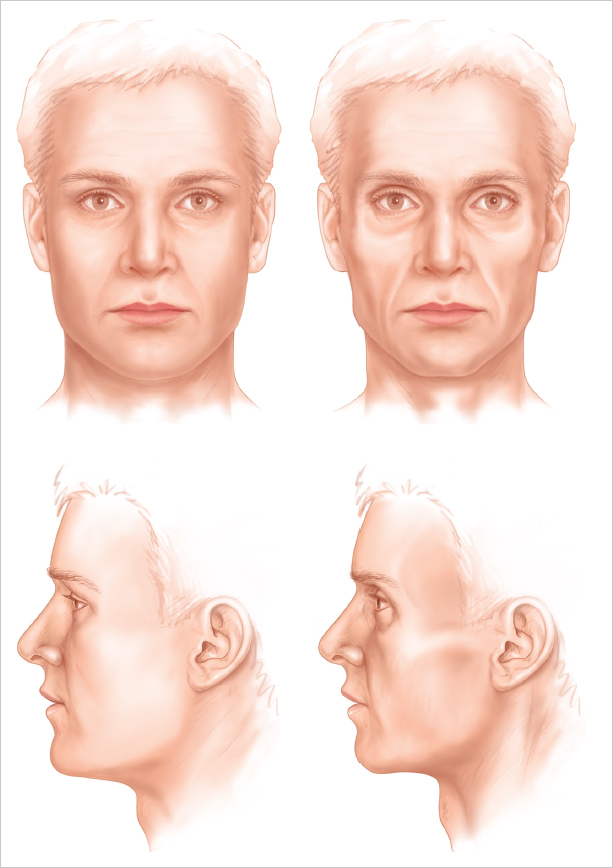
Among individuals with drug-related lipodystrophies, we have an unusual opportunity to observe facial atrophy. These patients give us a new appreciation of how people look when they lose facial fat. They do not necessarily look old; they look sick or anorexic from loss of subcutaneous fat. The areas of fatty tissue loss are specific: the cheeks and temples are most involved. The lips and perioral region out to the nasolabial fold are almost entirely spared in lipoatrophy. However, the cheek, from the malar region to the buccal region, and extending down into the area of the jowls, shows a marked loss of almost all soft-tissue fullness. As a person approaches middle age, the fat deposits of the jowl, above the nasolabial folds, in the eyelids, and so forth become more visible as their surrounding fullness disappears. Not only do the fat deposits become more obvious, but also many of the underlying structures of the face, such as the submaxillary glands and the bony skull, are more discernible as separate entities 7 ( Fig. 14.1 ). How each area of the face ages is discussed in great detail throughout this section of the book, but in almost all areas of the face the fat remains, along with bony structures, glands, and vessels, and the inherent fullness of youth disappears. And, of course, all of those changes are accompanied by a deterioration in the quality of skin over time, with the loss of skin thickness and elasticity.
Supraorbital Area
Usually, the primary problem with the aging forehead is not a contour deformity but the action of the frontalis muscle as it becomes less opposed by the diffuse fullness of youth. This results in wrinkles or creases that are created by intrinsic tone of the frontalis and other muscles.
Just as the fullness of youth projects health, the absence of fullness warns the observer of sickness, age, or starvation. The upper eyelid or brow area is one of the first areas to project deteriorating health. Just 1 or 2 mm of hollowness at the upper eyelids and temples can have a dramatic impact on how well a person looks.
The amount of upper eyelid visible under the brow can be variable in youth; the most frequent presentations are of the skin touching the eyelashes (with no eyelid visible) or with only 1 or 2 mm of palpebral show. A young, healthy person can occasionally present with deep-set eyes, but rarely with hollow eyes.
The eyebrow is supported laterally by temporal fullness. It is that temporal fullness that allows one to see the lateral quarter of the eyebrow in a youthful face and that supports the eyebrow into its lateral arch. The temporal fullness and lateral frontal fullness also produce the smooth, strong brow essential to a youthful appearance.
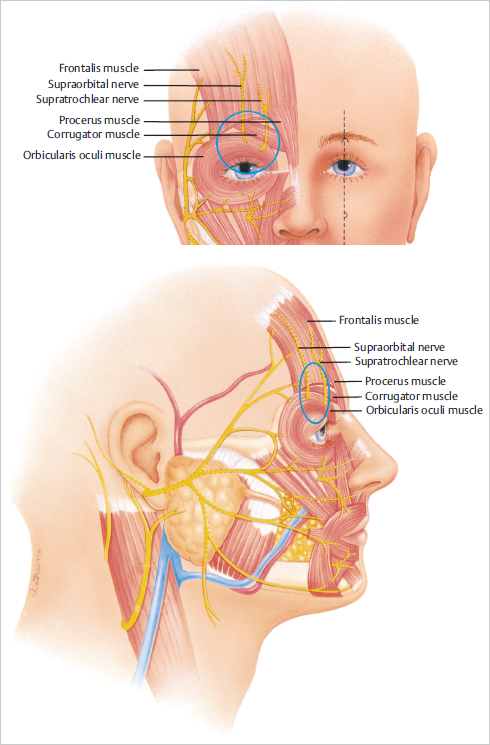
A thorough knowledge of the anatomy of the upper eyelids, brow, and temple is essential for the surgeon operating on the upper third of the face. Preventing injury to nerves and avoiding inadvertent cannulation of arteries or veins are primary concerns 7 ( Fig. 14.2 ).
Nose
The aging nose loses fullness in the glabella and nasion more than in any other location. As this area atrophies, the remaining parts of the nose become relatively larger. Therefore, the tip appears larger with the atrophy of the upper nose and tip. As this happens, the tip may also appear to plunge.
The most obvious and simplest use of fat grafting to the nose is to fill in irregularities and divots.
Nasolabial Fold
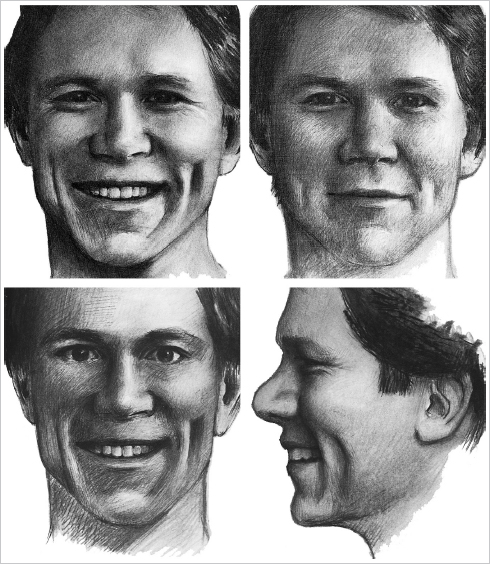
The topical anatomy of the nasolabial and marionette folds can vary greatly from individual to individual. At one end of the spectrum, they are almost completely absent or flat. At the other end, there is a prominent fullness lateral to the nasolabial fold with a pronounced premaxillary deficiency. The folds and the surrounding skin should be carefully evaluated when a fat grafting procedure is contemplated 14 ( Fig. 14.3 ).
The nasolabial folds and marionette grooves are strongly influenced by the surrounding structures in the cheeks, lips, and chin. In a younger person, the nasolabial folds and marionette grooves may be manifest as deep creases surrounded by fullness. In such situations, the folds may not project any particular negative emotion in spite of their prominence.
Chin/Jawline
The contour of a young, healthy chin has a distinct shape consisting of two distinct lateral protuberances with a central flattening or a cleft. I refer to this topographic relationship as the “ball–ball” of the chin. The lateral bulges project forward more than the central flattened or depressed area; thus, it is the lateral chin that establishes the anterior projection of the chin.
The distance between these two “balls” determines the shape of the chin. When they are close together, a more pointed chin results, with less flattening of the midline. When the prominences are far apart, as is typical in a young man, the separation creates a more angular chin with more midline definition. In many cases, the midline definition can result in a cleft, especially in younger chins.
The chin ages primarily by losing lateral and inferior fullness while retaining central fullness. As lateral and inferior volume is lost from the aging mentum, a “button” emerges in the upper middle chin area. This residual central bulge projects forward on the chin to become the most anterior point of the aging chin. As the volume from the lateral and lower chin is lost, the chin becomes more pointed, and the youthful curvature of the lower chin flattens out in an oblique path, dropping off from the new central point of projection down to the submentum. As the youthful fullness of the chin is lost, the chin’s thin skin falls into creases.
Mandibular Border
The young, healthy masculine mandibular border is full and strong and has a distinct lateral fullness cephalic to the most caudal extent of the border. It is this lateral fullness that is especially prominent posteriorly that catches the light to create a strong jawline shadow from the angle to the chin.
As in the rest of the face, generalized fullness between the skin and bones is lost with advancing age. As that underlying fullness is reduced, the face deflates. The enveloping sack of skin remains the same size, but without the underlying fullness and support. The emptied skin drapes around the underlying structures of the face exposing the facial muscles, the skull, and many pockets of fat. This is a generalized loss of subcutaneous fullness, not a loss of fat.
A glance behind the mandible at the aging earlobe reveals a similar loss of volume, only with a different type of deflation. The earlobe resembles an empty balloon that hangs; this is a clear example of descent directly following atrophy.
Aging of the soft-tissue covering of the mandible is a more complex process, but the primary mechanism is still deflation and radial entropy. As the soft tissues that frame the jawline disappear, the definition of the jawline becomes blunted. Without the lateral projection of fullness, the angle of the mandible loses its distinct shadow and appears to melt from the buccal region into the neck.
The largest collection of fat in the mandible is located at the jowl. This collection of fat is tethered with ligamentous attachments anteriorly. As the soft-tissue fullness of the entire mandible recedes, the fat of the jowl, which was formerly obscured by surrounding fullness, emerges. In other words, the fat of the jowl and the skin are the most obvious stable soft-tissue elements of the mandible, and the rest of the lower face disappears around it. The jowl does not descend, but instead the border of the mandible ascends, leaving the jowl below. Thus, the face does not get longer but shorter with age. It effectively shortens from the lateral and oblique views.
A full, taut neck is one of the signs of youth and beauty. Even though deep transverse cervical creases may be present in youth, deep horizontal folds in the neck are usually considered undesirable at any age. With age, the cervical subdermal fullness disappears and the skin texture gradually deteriorates, leaving behind unsupported, crepey skin. When structural fullness is added to the neck, it provides underlying support to the skin to restore a more youthful fullness. Recontouring of the neck with structural fat can provide further enhancement by disguising prominent neck cartilages.
Individuals with noticeable loss of subcutaneous fullness of the neck and apparent crepiness and thinning of the skin are the best candidates for neck rejuvenation with fat grafts. Unfortunately, the change that occurs with restoring structure to the supporting matrix of the neck is not as dramatic as in the face or even the hands, and the patient should not expect dramatic changes—only subtle improvement in texture and contours.
Many patients are bothered by prominent neck cartilages, either as a result of aging or because they feel that their Adam’s apple makes them look too masculine, even at a younger age. These patients usually seek softening of the prominent cartilages with three-dimensional volume placement around the cartilages. Another indication in younger patients is deep transverse neck creases.
As the jawline softens and retreats upward, the submental contents are exposed. The submaxillary gland and digastric muscles do not descend, rather the jawline ascends to expose them. Likewise, as the jawline narrows with loss of fullness, the structural support that distracted the lower face laterally dissipates. A lack of support provided by the radial expansion by the soft tissue over the mandible allows the unsupported skin to be pulled downward by gravity. This downward movement is almost entirely secondary to a loss of radial support.
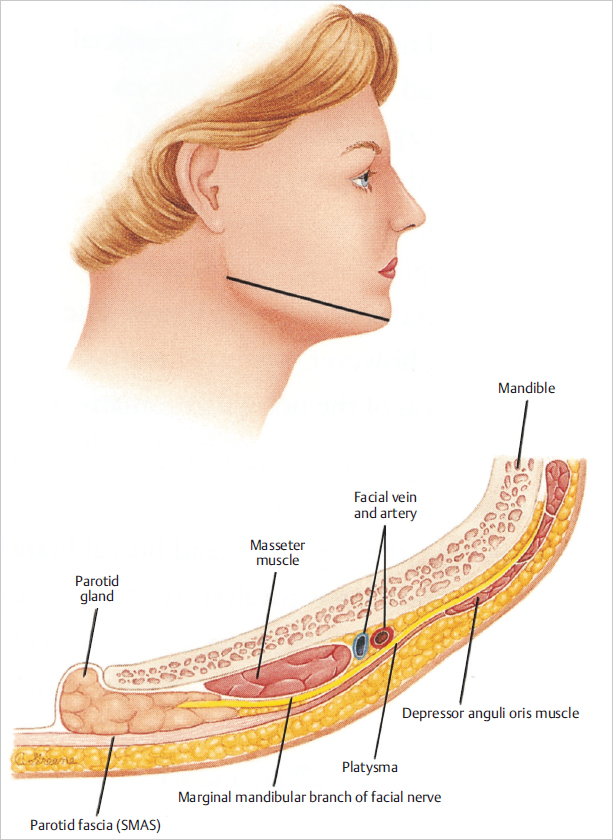
With regard to surgical considerations, the position of major salivary glands, the marginal mandibular branch of the facial nerve, the submental nerves, and the facial artery should be noted 14 ( Fig. 14.4 ).
Patient Selection
Fat Viability
To obtain long-term survival of transplanted autologous fatty tissue, the harvested and processed fatty tissue parcels must remain viable before implantation. Although several studies were performed in the past searching for improvement of fat transfer, 15 , 16 , 17 the viability of fat grafts harvested and processed by a number of techniques remains essentially less well known. Recently, several experimental laboratory tests including immunohistological staining have been used to determine the viability of fat grafts; the search for the best test to evaluate the viability of fat grafts continues 7 ( Table 14.2 ).
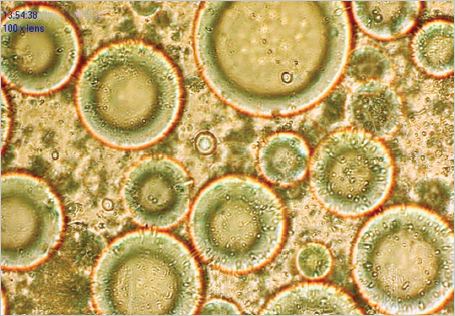
Laboratory tests that have been used to determine the viability of fat grafts include viable adipocyte counts, colorimetric assays, adipocyte-specific enzyme assays, routine histological examination, and immunohistochemical staining 7 ( Fig. 14.5 ). Each test must be processed in vitro and may be time consuming; each has been selected by investigators as a single test or in combination to determine the viability of fat grafts experimentally.
It is essential that fat grafts harvested and processed by whatever technique maintain their viability before they are transplanted in patients. Our recent study favors the Coleman technique as a preferred method for fat graft harvesting and processing, because this technique yields a greater number of viable adipocytes and sustains a more optimal level of cellular function within harvested and processed fat grafts. 18
Source: Adapted from SR Coleman, RF Mazzola, LLQ Pu. Fat Injection: From Filling to Regeneration. 2nd ed. New York, NY: Thieme; 2018.
Steps for Facial Fat Grafting
Preoperative Considerations
On the day of surgery, the blueprints are reviewed and the plan discussed again with the patient. Patients almost always have questions that have not been answered at previous consultations or by the support staff. The patient reads and signs the operative consent form that delineates the planned procedure in words he or she can understand.
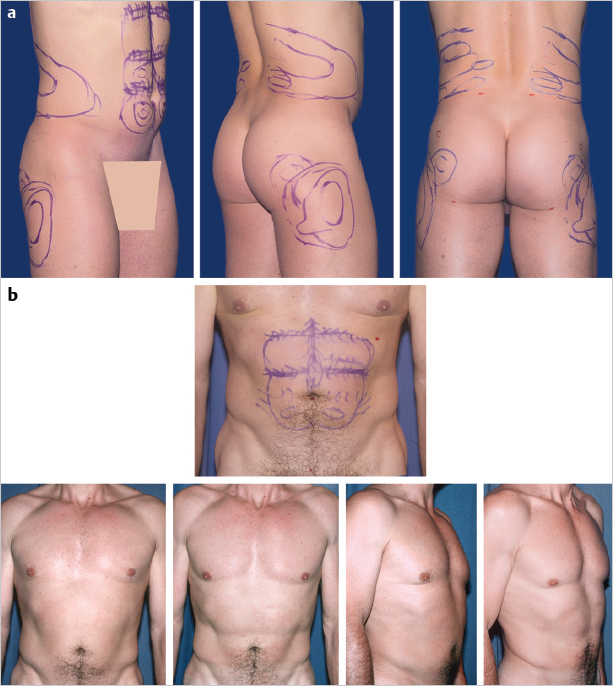
On the day of the procedure, colored marks (Penmark laundry markers work well) are drawn on the patient’s face using the blueprints created at the second consultation as guides. The markings outline both the areas to be augmented and the amount of tissue to be infiltrated. The markings can be used to remind the surgeon of the specific levels of placement against the skin, against bone, or in intermediate levels.
I use colors similar to those used in the tracings, with the exception of yellow, because it is difficult to see on the face during the procedure. Green marks the locations for structural changes, and orange delineates where no fat will be placed. From the green marks to the orange marks will be a transition or feathering zone. I use purple to indicate special considerations, such as the purple diamonds on this patient’s cheeks, which designate the proposed height of the cheek. I also use purple to show areas of removal of fatty tissue. Finally, I use the color red to denote incision sites.
Harvesting Fatty Tissue
The surgeon must adhere to sound surgical principles when harvesting and preparing subcutaneous tissue for autotransplantation. Fatty tissue is more fragile than most other kinds of human tissue. Fatty tissue was never intended to survive unprotected. Outside the body, fat is easily damaged by mechanical, barometric, and chemical insults. To survive harvesting, transport, and implantation, fat must be harvested in intact parcels small enough to be inserted through a small cannula but large enough that the tissue architecture is maintained.
The material harvested by syringe liposuction may contain as little as 10% or as much as 90% fatty tissue. The aspirated material separates into three layers on centrifugation: the top layer is composed primarily of oil, the bottom layer is almost entirely blood and lidocaine, and the middle layer is potentially viable fatty tissue.
Because I have observed no clear correlation between donor site location and longevity of implanted tissues, I select harvesting sites that enhance body contour and are easily accessible in the supine position. The abdomen and medial thighs are most commonly used 14 ( Fig. 14.6 ).
Meticulous sterile technique is always observed with careful attention to preoperative patient preparation with antiseptic soaps and an antiseptic agent such as povidone–iodine.
The choice of anesthetic agent for harvesting depends on the donor areas and the projected volume of fat to be removed. For smaller harvesting volumes, a local anesthesia using 0.5% lidocaine with 1:200,000 epinephrine is adequate.
An epidural or general anesthesia is preferred for removal of larger volumes or when multiple sites are used.
Instrumentation
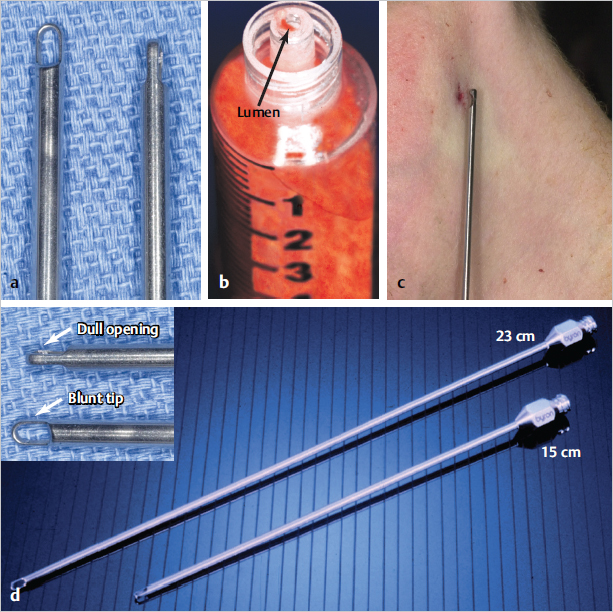
A blunt-holed cannula with nine distal openings is used for harvesting 14 ( Fig. 14.7a,b). The tip of the cannula is completely blunt and is shaped like a bucket handle. The other end of the cannula is attached to a 10-cc Luer-Lok syringe. Parcels that can pass through the lumen will usually pass through the much smaller lumen (17-gauge) of the infiltration cannulas without clogging (Fig. 14.7c,d).
Technique
Fatty tissue is harvested through the incisions made for infiltration of anesthetic solutions. These incisions are just large enough (usually 2–3 mm) to permit the insertion of the tip of the harvesting cannula.
Attach the cannula to a 10-cc Luer-Lok syringe. Pull back the plunger gently to minimize negative pressure. Never use a plunger-locking device. If substantial fluid is present, the syringe is placed on a table for several minutes to allow the fatty tissue to separate. Then, the aqueous portion can be expressed by pressing on the syringe.
Close all incision sites with nylon interrupted sutures.
Refinement and Transfer
Intact parcels of fatty tissue can withstand brief centrifugation. “Washing” of the harvested tissue is not recommended. It exposes the reticular fibers and connective tissue to unnecessary trauma. Avoid exposure of the fatty tissue to the open air.
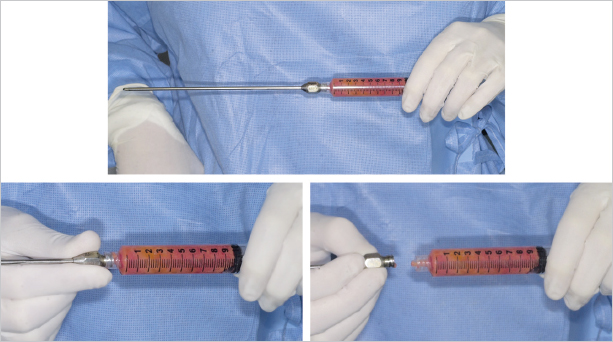
After the fat has been harvested, the cannula is removed from the syringe and replaced with a plug. The plug is twisted on to create a seal that will prevent spills during the centrifuging process 14 ( Fig. 14.8 ).
The syringe without the plunger is then placed into a centrifuge to separate the viable from the nonviable components. The recommended centrifugation is at 3,000 rpm for 3 minutes 14 ( Fig. 14.9 ).
Once the rotor of the centrifuge has stopped, the circulating nurse should open the cover, and the sterile technician should remove the centrifuged syringes 14 ( Fig. 14.10 ). The fatty tissue is separated into three levels:
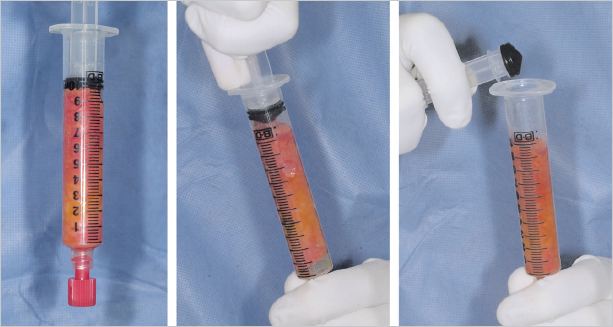

The upper level is less dense and is composed primarily of oil, presumably from ruptured cells.
The middle portion is composed primarily of potentially viable parcels of tissue.
The lowest level is the densest layer and composed primarily of blood, water, and lidocaine.
Decant the oily layer before removing the plug from the Luer-Lok syringe. After the oil is decanted, the plug can be removed. A collection vessel should be handy as the aqueous component will usually pour out of the syringe.
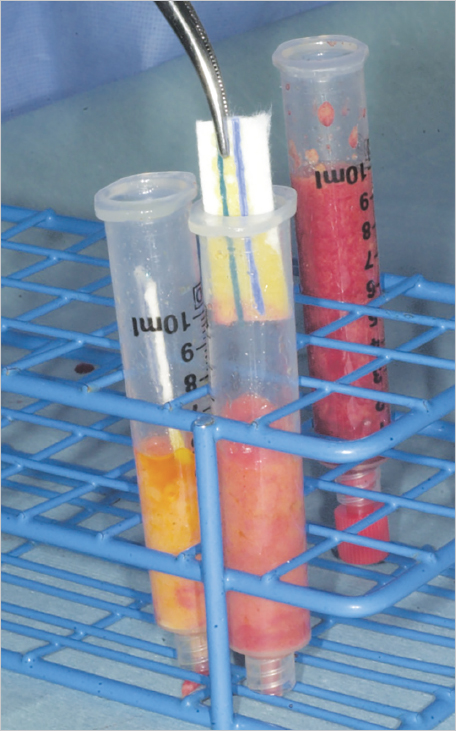
Wick the most superior portion of the harvested fat with Codman neuropads that can make removing the oily component easier. After 4 minutes, the wick is replaced with another neuropad. Wicking is performed at least twice 14 ( Fig. 14.11 ).
Replace the plunger after allowing the fatty tissue to slide down to the edge of the syringe. The fat can be stored in the syringe for brief periods of time before transferring into smaller syringes for infiltration.
Transfer the fat into smaller syringes. Use 1-cc Luer-Lok syringes to place tissue into the face and hands. The plunger is replaced and advanced to remove dead space. The refined fat is now ready for infiltration.
Clinical studies have demonstrated improved survival of grafted fat after centrifugation. A study from Japan emphasized the importance of concentrating stem cells in the fat to enhance graft take. 19 Another study from Germany has confirmed that the growth factors are isolated and present in greater numbers in centrifuged fat; they also do not migrate into the aqueous or oil fractions. 20
A few years ago, it became obvious to me that different levels of centrifuged fat are probably composed of different cellular and biological elements. Obviously, the upper level of centrifuged fat is oilier and less dense, whereas the lower level is much denser and less oily. Begin using the denser fat preferentially in areas that require more predictable results and avoid the use of the less dense, oilier-appearing fat. We undertook a study at New York University to evaluate the different densities of centrifuged fat and found that the high-density centrifuged fat survived to a greater extent with less fibrosis than low-density fractions. In addition, the high-density fraction had much greater stem cell activity and a greater concentration of growth factors. 21
With this knowledge in hand, I now approach fat grafting differently. The normal yield from 10 cc of harvested fat is 4 to 6 cc of refined fat. If I have that yield, I segregate out the lowest 2 cc of fat to use preferentially to increase survival and predictability.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


