Chapter 12 THE PHYSIOLOGY OF INJURED, OBESE, GRAFTED, AND DYING FAT
Physiologically, adipose tissue turns over very slowly, although thousands of adipocytes die and are replaced with next-generation adipocytes every second. Besides physiologic remodeling, accidental remodeling occurs from various kinds of tissue damage, including trauma, ischemia or hypoxia, application of mechanical force, and inflammation. Harvesting fat for fat grafting by liposuction causes traumatic damage to the donor site, while dynamic tissue remodeling of grafted fat (degeneration and regeneration) occurs in the recipient site. By scientifically exploring the cellular event after fat grafting, investigators can pursue strategies to improve the clinical outcomes of fat grafting, such as tissue volumization, revascularization, and revitalization of adipose tissue.
The Role of Adipose-Derived Stem Cells in Adipose Tissue Remodeling
Adipose-derived stem cells (ADSCs) are the main cell population contributing to adipocyte generation or regeneration in any types of adipose tissue remodeling or expansion (see Chapter 6) such as developmental growth, hyperplasia in obesity, repair processes after injury or ischemia, 1 or tissue expansion induced by internal or external mechanical forces. 2 These remodeling processes are in balance between adipocyte apoptosis or necrosis and adipogenesis, managed by ADSCs. Subcutaneous adipose tissue has the highest tissue partial oxygen tension (pt O2; 40 to 60 mm Hg) among all body organs. The high pt O2 of adipose tissue probably reflects the high density of capillaries and low oxygen consumption rate of the tissue. Diabetic adipose tissue is relatively ischemic, contains occasional dead adipocytes, and exhibits low-grade chronic inflammation, which causes adipose endocrine dysfunction, insulin resistance, and metabolic syndrome. In contrast, lipomatous tissue is not ischemic, probably as a result of upregulated angiogenesis. 3
Among the cellular components of adipose tissue, adipocytes are most susceptible to death under ischemic conditions such as 15 mm Hg of pt O2. 4 When severe ischemia is prolonged, adipocytes die first within 24 hours, and vascular endothelial cells and blood-derived cells start to die next. In contrast, ADSCs can remain alive up to 3 days even under severe ischemia 4 ; rather, during the 3 days, ADSCs are activated by signals released from dying cells and contribute to the adaptive repairing process, such as adipogenesis and angiogenesis, usually with collaboration with other stem/progenitor cells recruited from bone marrow. 4 , 5
In jury to Adipose Tissue
Adipose tissue injury induces tissue damage and follows the repair process, which involves recruitment of inflammatory cells and release of inflammatory cytokines. After injury, degenerative changes such as adipocyte death occur, and primary injury factors such as basic fibroblast growth factor (bFGF) and some factors released from aggregated platelets such as platelet-derived growth factor (PDGF), epidermal growth factor (EGF), and transforming growth factor-beta (TGF-beta) are first released into the injured site and trigger a cascade of wound healing processes. 1 , 6 Basic fibroblast growth factor (FGF) is released from damaged connective tissue and acts through a c-Jun N-terminal kinase (JNK)–signaling pathway to stimulate quiescent ADSCs not only to proliferate but also to secrete secondary growth factors, such as hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF). Thus ADSCs contribute to the regeneration of adipose tissue and suppression of fibrogenesis during the first week after injury. 6 In parallel, a variety of stem or progenitor cells such as endothelial progenitor cells (EPCs) are recruited from bone marrow and collaborate with activated ADSCs in an orchestrated repair of the damaged adipose tissue.
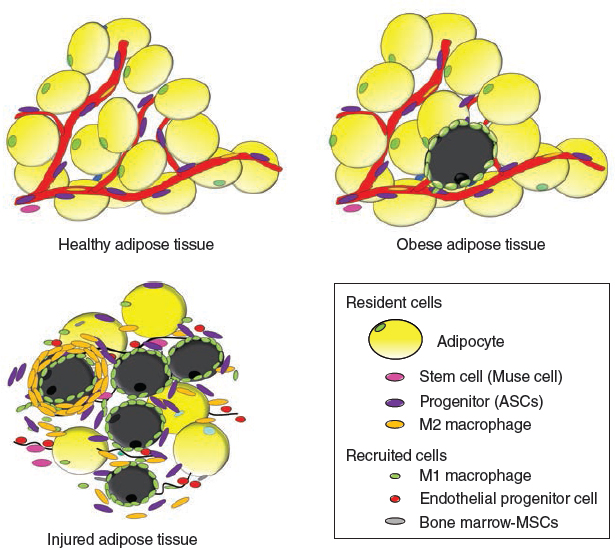
Intact adipose tissue has adipocytes as well as many other types of cells such as adipose-derived stem/stromal cells (ADSCs) and vascular endothelial cells (VECs). Obese adipose tissue occasionally has dead adipocytes surrounded by infiltrated M1 macrophages (crownlike structures) and shows low-grade chronic inflammation. When adipose tissue is injured, ADSCs are activated and many types of progenitor or stem cells are recruited from bone marrow to repair the tissue damage.
Mechanical Forces and Adipose Tissue
Mechanical forces, whether external (shear, stretch, tension, distraction, and compression) or endogenous (generated within the active cytoskeleton), affect tissue growth and cellular functions. Moreover, physical interactions between ADSCs and the extracellular matrix influence the cell behaviors. 7 Continuous external tissue expansion (as with the BRAVA system) can be used for the expansion of breast tissue. 8
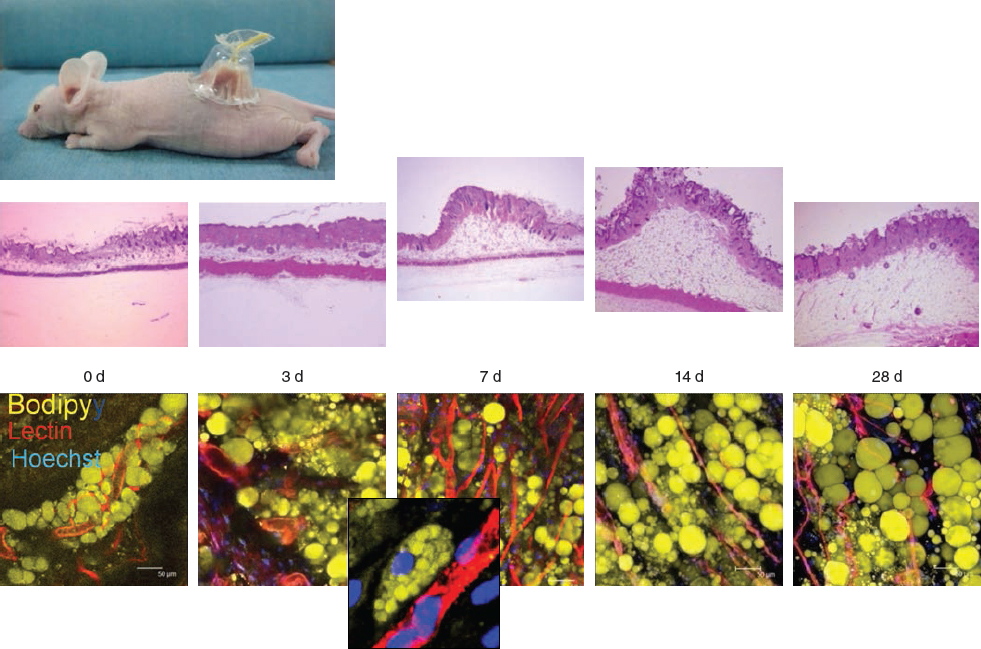
We performed an experiment in mice in which 4 weeks of external expansion caused an increase in subcutaneous tissue volume, particularly adipose tissue, although the enlargement was reversed 2 weeks after the removal of the device. 2 Dynamic remodeling such as adipogenesis and angiogenesis in the direction of the mechanical force was seen over time. The regenerating potential has been attributed to the number (density) and potential of ADSCs; thus irradiated tissue would have a very limited potential for expansion.
What Happens After Fat Grafting?
Recently, rigorous efforts in basic animal studies have been undertaken to explore the mystery of fat grafting; these have revealed the underlying cellular mechanisms regarding how the grafted fat behaves. Grafted fat is a nonvascularized tissue, and only superficial cells can survive, as in a skin graft. Although most other cells in the graft die, the degenerated tissue can be partly regenerated as a result of the contribution of ADSCs and other stem/progenitor cells.
In the regenerating zone, the hypoxic condition was improved by revascularization within 3 days after grafting and ADSCs gave rise to new adipocytes, which finally replaced the dead adipocytes by 3 months. On the other hand, in the necrotizing zone, the microenvironment was not improved within 3 days, and thus ADSCs finally died, leading to the central necrosis of the graft tissue.
ACUTE EVENTS IMMEDIATELY AFTER FAT GRAFTING
Once injected into the recipient site, the adipose tissue is in an ischemic (hypoxic) state and is nourished only by plasmatic diffusion from the surrounding host tissue for a few days until revascularization occurs. This results in the death of many adipocytes within 24 hours and the release of multiple cell death- or injury-associated factors from both the dying grafted tissue and the injured host tissue. 4 , 6 Inflammatory cells such as macrophages and lymphocytes are infiltrated, and inflammatory cytokines such as interleukins are secreted. Despite the death of adipocytes, ADSCs, which can remain functional up to 72 hours, even under severe ischemia, are activated and try to repair the damaged tissue in collaboration with infiltrated stem/progenitor cells recruited from bone marrow. 4 , 5
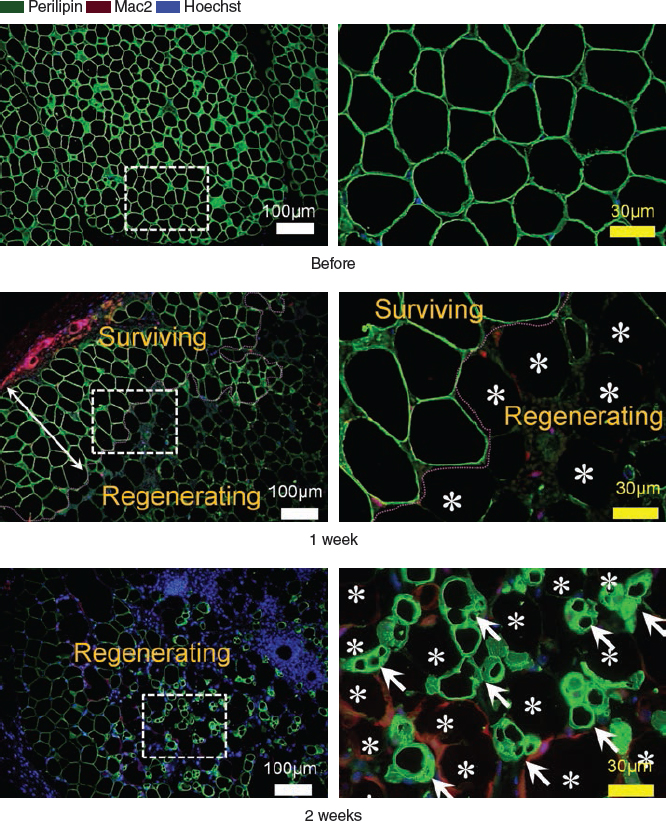
In this study of the immunohistology of grafted fat tissue in mice, harvested tissue samples were immunostained for perilipin (cytoplasm of viable adipocytes, green), Mac2 (monocytes/macrophages, red), and Hoechst 33342 (nuclei, blue). 5 Rectangles in the low magnification images (left column) were further magnified (right column). The demarcation between the surviving and regenerating zone became clear at 1 week (dashed line); dead adipocytes (*) were perilipin negative, and surviving adipocytes were strong-positive for perilipin. Small-sized preadipocytes with multiple intracellular lipid droplets (arrows) emerged between dead adipocytes at 2 weeks; the dead adipocytes were surrounded by a single layer of M1 macrophages (stained red).
Related posts:
 Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
Chapter 11 THE EVOLUTION OF ADIPOSE BIOLOGY AND REGENERATIVE MEDICINE
 Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
Chapter 13 ADIPOSE TISSUE IN WOUND HEALING
 Chapter 14 PLATELET-RICH PLASMA AND FAT GRAFTING
Chapter 14 PLATELET-RICH PLASMA AND FAT GRAFTING
 Chapter 15 CRYOPRESERVATION OF ADIPOSE TISSUE FOR FAT GRAFTING
Chapter 15 CRYOPRESERVATION OF ADIPOSE TISSUE FOR FAT GRAFTING
 Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
Chapter 23 SIMULTANEOUS FACELIFT AND FAT GRAFTING: COMBINED LIFTING AND FILLING FOR REJUVENATION OF THE AGING FACE
 Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Chapter 36 AUGMENTATION OF THE BREAST AND TUBEROUS BREAST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


