CHAPTER 11 Submental Contouring
Summary
Submental contouring of the aging neck incorporates a number of essential techniques to markedly improve neck definition and appearance. Thorough patient evaluation is essential; factors related to neck skin condition, degree of submental adiposity, platysmal muscle laxity, muscle banding, position of the hyoid–thyroid cartilage complex, jowling, submandibular gland ptosis, and overall shape of the chin must be carefully analyzed to appropriately counsel patients, provide them with realistic expectations, and effectively produce outcomes. Generally, male patients may be less inclined to undergo a combined face-lift procedure to avoid a feminized look. In these cases, the surgeon may offer alternate options that effect changes in neck rejuvenation alone such as submental liposuction, cervical lipectomy, platysmal plication, and/or direct cervicoplasty. This chapter highlights the technical details of submental contouring while discussing neck anatomical details, which contribute to decision making and surgical outcomes.
Introduction
The techniques of submental contouring and efforts to rejuvenate the aging neck have garnered much interest in the last half century. As early as the 1960s, Millard et al. 1 described direct submental lipectomy and excision of hypertrophic anterior platysmal bands through a small submental incision. A decade later, Schrudde 2 described the concept of “lipexeresis” in his attempts to contour the thigh and knee by fat curettage. Since then, others have suggested fat removal through tubes attached to suction devices. Ilouz, in particular, described a technique of njecting saline into the proposed surgical site and using a blunt-tipped cannula for fat aspiration and lipolysis in the context of body and submental contouring.
Over the years, other techniques have become incorporated into neck rejuvenation, with Connell 3 describing a technique of combining submental lipectomy with platysmal band resection and platysmal sling creation to improve the neck contour. Suture suspension techniques led to the concept of corset platysmaplasty, described by Feldman 4 in 1990. These maneuvers, combined with liposuction, have added to the facial plastic surgeon’s armamentarium of creating the most aesthetically pleasing neck contour.
Physical Evaluation
Assess the patient’s overall health condition and inquire about systemic medical factors that could negatively impact wound healing (presence of diabetes, uncontrolled hypertension, coagulopathy, connectivetissue disorders, smoking or nicotine use, and use of anticoagulants or immunosuppressive medications).
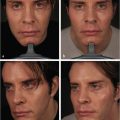
Evaluate the patient in an upright position in a room with ample lighting. Take photographs for before and after comparisons.
Perform a complete facial examination in conjunction with evaluation of the neck and submental area.
Assess the neck and facial skin condition (overall skin quality, tone, propensity for hypertrophic scarring or keloid formation, degree of chronological aging and photoaging, thickness, elasticity, laxity, wrinkling, and pigmentary changes).
Palpate the degree of submental adiposity.
Assess laxity of the platysmal muscle as well as the presence of muscle bands.
Determine the cervicomental angle by relating the position of the hyoid–thyroid cartilage complex to the mandible.
Evaluate for the presence and degree of submandibular gland ptosis.
Assess presence of jowling and melolabial folds. These can influence the overall postsurgical appearance of the face and neck.
Evaluate the shape of the mandibular bone as well as the position and projection of the chin to determine whether a mentoplasty could improve the overall aesthetic appearance.
Anatomy
The neck can be separated into two separate (anterior and posterior) triangles, with the focus on the anterior triangle during a submentoplasty. The midline of the neck is delineated by the trachea, thyroid, and cricoid cartilages. The superior border of the anterior triangle is lined by the chin and mandibular border. Between the skin and platysma lies the subcutaneous fat, with most of the volume positioned in the anteromedial region. The degree of platysmal fiber decussation will determine how much of the subcutaneous fat is contiguous with the subplatysmal fat. Because this fat is void of fibrous connections and septations, it is more amenable to sculpting through either liposuction or lipectomy.
The paired platysma muscles are contiguous with the superficial muscular aponeurotic system and course from an inferolateral to superomedial direction. The degree of muscle decussation in the midline of the neck is variable, depending on factors like genetics and aging. Over time, the platysma loses tone, and the deep retaining ligaments on the medial edges of the muscle become attenuated; this allows for the following:
Herniation of interplatysmal fat.
Lateralization of the muscle edges.
Platysmal band development.
All of these can contribute to neck aging, submental fullness, and a more obtuse cervicomental angle. Removal of submental adipose tissue and plication of the muscle edges help mitigate these changes.
The sternocleidomastoid (SCM) muscle defines the lateral boundary of the anterior triangle. The external jugular vein and greater auricular nerve run along the lateral aspect of the SCM, separated from it by the investing layer of the deep cervical fascia. The greater auricular nerve crosses the SCM at Erb’s point, at the junction of the superior third and lower two-thirds of the muscle. As the neck dissection extends posterolaterally, it is important to work in a plane superficial to the fascia of the SCM to prevent injury to the vein or greater auricular nerve.
The digastric muscles have been thought to contribute to the formation of the cervicomental angle, and various efforts have been made to modify the muscles to help with rejuvenating the aging neck. Some advocate for muscle plication or resection of the anterior digastric muscle bellies while others discuss releasing the suprahyoid tendon aponeurosis. Submandibular gland ptosis is another factor that should be noted.
One crucial step in the physical examination of a facial rejuvenation patient is evaluating the position of the hyoid. The relationship of the hyoid bone position to the mandible corresponds with the cervicomental angle; a more inferiorly positioned hyoid will produce the appearance of an obtuse angle. This observation is important to elucidate to the patient preoperatively as well, as an inherently low anatomical position can limit optimal postoperative results.
In highlighting the differences between male and female neck rejuvenation, some males may be less inclined to undergo a combined face-lift procedure to avoid a feminized look. Surgical plans to address the excess submental adiposity, skin laxity, and platysmal banding will need to be tailored with the male anatomical characteristics in mind. This will help the surgeon achieve the most natural-appearing results.
One option that is more amenable for men is a direct cervicoplasty, which includes resection of submental skin in combination with lipectomy and platysma plication.
Patient Selection
Patient neck and facial attributes must be carefully and methodically analyzed prior to recommending surgical options for submental contouring. The patient should be asked about any relevant prior rejuvenation procedures he or she has undergone such as radiofrequency treatments, noninvasive lipolysis, injection lipolysis, and previous surgeries. Review the patient’s history and evaluate for any systemic medical factors that could negatively impact wound healing and preclude the patient from achieving optimal results. Medication lists should be reviewed thoroughly, and patients taking anticoagulation medications should discuss with their primary care physicians about temporarily suspending them to help limit the potential for postoperative complications. Although some surgeons may not agree to proceed with surgery for those who actively smoke or use tobacco products, those who do should have candid discussions with their patients about the potential for increased wound complications.
Steps for Submental Liposuction in Men
Incision
In a natural submental crease, use a marking pen to design a 2- to 3-cm incision. This incision should be wide enough to accommodate a retractor and to allow visualization of the neck dissection ( Fig. 11.1a,b). The crease should be injected with local anesthesia (we use 1% lidocaine in 1:100,000 epinephrine) ( Fig. 11.1c). Local anesthesia should be injected with a 25-gauge spinal needle to the subcutaneous tissues. A No. 15 blade is used to make the submental skin incision. Monopolar diathermy is then used to dissect through the subcutaneous tissue.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


