CHAPTER 1 Lymphedema: Lack of Solutions to a Clinical Problem
KEY POINTS
There is no fully satisfactory treatment for lymphedema.
Current treatment is compressive or surgical.
Decongestant therapy is the benchmark of conservative treatment.
Surgery has traditionally been excisional.
More recent surgery includes bypass operations (lymphaticovenular anastomoses) and vascularized lymph node transfer.
Lymphedema is a progressive, chronic condition that affects a significant number of people and can have deleterious effects on the physical and psychosocial health of the patient. Lymphedema, which is especially common after surgical treatment for malignancy, has traditionally been viewed as incurable or refractory. The precise cause of lymphedema is still not completely understood, and this has led to undertreatment and misdiagnosis.
Even though lymphedema may be greatly ameliorated by appropriate management, many patients receive inadequate treatment, are unaware that treatment is available, or do not know where to seek help. Several recent systematic reviews have highlighted the distinct lack of evidence for the optimal management of lymphedema. 1 – 3 There are nonsurgical options, also known as conservative treatment, that have remained unchanged for many years despite occasionally cumbersome regimens and average results. Surgical options, which include ablative operations, liposuction, and physiologic operations, have also been used, with mixed results. Despite advances in microsurgery, there is neither consensus on surgical or nonsurgical procedures nor a standardized protocol in the treatment of the patient with lymphedema.
Given the lack of consensus on one particular avenue of treatment for lymphedema, the lymphedema practitioner must have multiple intervention options available. This book will present the latest information on the diagnosis, treatment, and management available in the field to allow the practitioner to best serve the patient. This chapter presents an overview of that information and the various solutions available to the lymphedema practitioner. The ultimate goal is to raise the profile of the condition and stimulate refined research and standardized treatment protocols to improve patient care.
Lymphedema: The Clinical Problem
Lymphedema is a chronic, debilitating condition that results in the disruption of the lymphatic transport system, which leads to the accumulation of protein-rich fluid in the interstitial space because of an imbalance between interstitial fluid production and transport (usually low output failure). Outside of the United States, the most common cause of secondary lymphedema is infection with the nematode Wuchereria bancrofti. This condition is also known as filariasis (see Chapter 15 for more on filariasis).
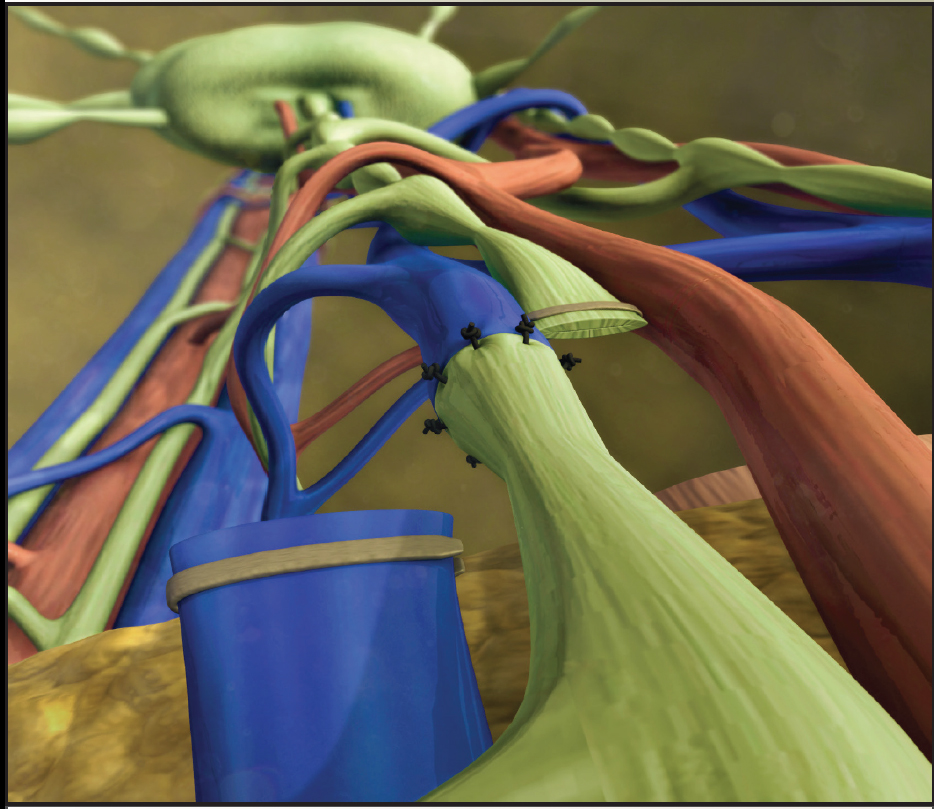
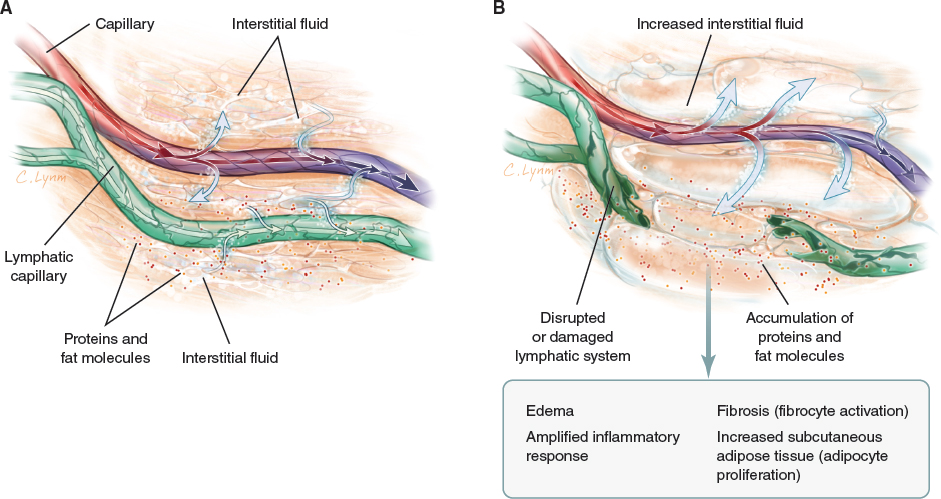
With obstructed or diseased lymphatic vessels, the accumulation of fluid gives rise to stasis of proteins and interstitial fluid. According to the Starling equation, increased protein concentration (Starling forces) results in increased colloid osmotic pressure in the tissue and a net gradient of fluid toward the interstitium. This physiologic phenomenon leads to edema, fat deposition of nontransported fat molecules, and fibrocyte activation as the result of an amplified inflammatory response. It is postulated that this triad of edema, fibrosis, and fat deposition is the supposed cause of lymphedema, although in reality this is more likely the effect than the cause. In patients with chronic lymphedema, large amounts of subcutaneous adipose tissue may form. Although incompletely understood, this adipocyte proliferation may explain why conservative treatment may not completely reduce the swelling and return the affected area to its usual dimensions (Fig. 1-1).
Lymphedema manifests as soft and pitting edema early in the disease and progresses to chronic induration, overgrowth, and disfigurement later on (Fig. 1-2). Lymphedema may manifest as swelling of one or more limbs and may include the corresponding quadrant of the trunk, in addition to other areas, such as the head and neck, breast, or genitalia. It is congenital, infectious, or iatrogenic, although the exact cause is still not fully understood.

Lymphedema is classified as either primary or secondary based on etiologic factors. Primary lymphedema is a congenital disease of the lymphatic system. It can present in infancy when it is known as Milroy disease. When it presents in adolescence, it is known as lymphedema praecox. Another manifestation presents when the patient is in his or her 30s and is known as lymphedema tarda. In primary lymphedema, lymphatic fluid collects in the subcutaneous tissues under the epidermis because of obstruction, malformation, or underdevelopment (hypoplasia) of various lymphatic vessels. Secondary lymphedema is an acquired disease of normal lymphatic vessels through either disruption or obstruction.
At birth, about 1 in 6000 people will develop primary lymphedema. The overall prevalence of lymphedema has been estimated at 0.13% to 2%. In developed countries, the main cause of lymphedema is widely assumed to be treatment for cancer. The incidence of lymphedema after breast cancer treatment ranges from 24% to 49% after mastectomy 4 – 8 and 4% to 28% after lumpectomy. 9 , 10 Patients requiring more aggressive surgery and radiation have a greater risk of developing lymphedema; however, the less invasive sentinel node biopsy is associated with only a 5% to 7% incidence of upper extremity lymphedema. 11 In addition to breast cancer treatment, treatment for other malignancies is also associated with lymphedema: melanoma (16%), gynecologic cancers (20%), genitourinary cancers (10%), head and neck cancers (4%), and sarcomas (30%). 12 However, it appears that about one quarter to one half of affected patients have other forms of lymphedema, including primary lymphedema and lymphedema associated with poor venous function, trauma, limb dependency, or cardiac disease. 13
The International Society of Lymphology has classified lymphedema into four stages based on certain clinical parameters 14 (Table 1-1). Pain and discomfort are frequent symptoms, and increased susceptibility to cellulitis can result in frequent hospitalizations and long-term dependency on antibiotics. 15 Lymphedema also causes hyperkeratosis, papillomatosis, erysipelas, lymphangitis, and the development of cutaneous tumors, such as Kaposi sarcoma, lymphoma, and even lymphangiosarcoma. 16 , 17 Increased limb size can interfere with mobility and affect body image. 18 – 20 In essence, lymphedema may produce significant physical and psychological morbidity. It is a chronic condition that presently is not curable but may be alleviated by appropriate management; if ignored, it can progress and become extremely difficult to manage.
Nonsurgical Management
The treatment of lymphedema is divided into nonoperative and operative methods. With both approaches, meticulous skin hygiene and care (cleansing, low pH lotions, and emollients) are vital to the success of virtually all treatment approaches. Basic range-of-motion exercises of the extremities, limb compression, and limb elevation are also helpful. Some studies support vigorous exercises under the correct conditions. However, little substantive data exist in the form of well-designed, case-control studies that compare methodologies. 14 It is clear that early treatment is optimal for the best outcome.
The best practice management of lymphedema involves a multidisciplinary approach that includes the following:
Exercise and movement: to enhance lymphatic and venous flow
Swelling reduction and maintenance: to reduce limb size or volume and improve subcutaneous tissue consistency through compression and/or massage
Skin care: to optimize the condition of the skin, treat any complications caused by lymphedema, and minimize the risk of cellulitis or erysipelas
Risk reduction: to avoid factors that may exacerbate lymphedema
Pain and psychosocial management
Swelling reduction is achieved through a combination of compression and exercise with or without lymphatic massage (manual lymphatic drainage [MLD] or intermittent pneumatic compression [IPC]). The precise regimen required will be determined by the site, stage, severity, and complexity of the lymphedema and the patient’s psychosocial status. Successful management of lymphedema relies on patients playing an active role in their care.
MANUAL LYMPHATIC DRAINAGE
MLD encourages fluid away from congested areas by increasing the activity of normal lymphatics and bypassing ineffective or obliterated lymph vessels. Although there is a wealth of clinical opinion advocating the benefits of MLD, massage alone does not appear to be beneficial. 21 – 23 Based on current evidence from 10 randomized controlled trials, there is little evidence to support the use of massage alone. 24 Furthermore, if performed overly vigorously, massage may damage lymphatic vessels. Deep, heavy-handed massage should be avoided, because it may damage tissues and exacerbate edema by increasing capillary filtration. The most appropriate techniques, optimal frequency, and indications for MLD, as well as the benefits of treatment, need clarification. MLD is a specialist skill that needs regular practice to maintain competence. (MLD is discussed in detail in Chapter 29.)
COMBINED PHYSICAL THERAPY AND COMPRESSION
Combined physical therapy (CPT), also known as complete or complex decongestive therapy, is also a two-stage treatment protocol. In phase I, the main goals are size reduction of the affected limb and improvement of the skin. After phase I, the patient with lymphedema proceeds to phase II, an ongoing, individualized, self-management phase to maintain the gains of phase I. 25
The goals of CPT are to:
Increase lymph drainage from the congested areas 28 , 29
Reduce skin fibrosis and improve the skin’s condition 30
Enhance the patient’s functional status 31
Relieve discomfort and improve quality of life 26 , 27 , 32 – 36
Reduce the risk of cellulitis and Stewart-Treves syndrome, a rare form of angiosarcoma 17 , 37
CPT is more labor intensive than other modalities, but its efficacy in reducing lymphedema is supported by long-standing experience. 38 , 39 It is considered the standard of treatment for several reasons. First, CPT uses skin care, manual lymph node drainage, range-of-motion exercises, and multilayer bandage wrapping. Multilayer bandage wrapping is the mainstay of conservative therapy. 40 Second, phase II maintains the results of phase I with the use of a low-stretch elastic stocking or sleeve compression. Compression alone has shown some benefit. Both multilayer inelastic stockings and controlled compression therapy (the garment’s size is tailored after edema volume changes) reduce edema volume by 31% 16 and 46%, 41 respectively. With CPT, randomized, controlled studies have shown a mean decrease of between 40% and 60% in edema volume. 21 , 42 , 43 Noncontrolled clinical trials demonstrate results similar to those of randomized trials. 27 , 44 – 47
Compliance is imperative for successful outcomes, and even with an actively participating patient, results vary. 46 The prerequisites of successful CPT are the active participation of the patient, availability of physicians, nurses, and therapists specifically educated and experienced in this method, health insurance coverage of the cost of treatment, and industry willingness to provide high-quality products. Compressive bandages, when applied incorrectly, can be harmful and should be placed by professionally trained personnel. Newer devices and garments are continuously being manufactured to reduce the bandage burden and improve compliance. However, the patient must understand that CPT is not a cure but only a risk-reduction strategy.
THERMAL THERAPY
Although combinations of heat, skin care, and external compression have been successfully used by practitioners in Europe and Asia for thousands of patients, the role and value of thermotherapy alone without compression or MLD in the management of lymphedema remain unclear without further rigorous comparative studies. 48 – 50
MEDICATIONS
Drug therapy to treat lymphedema has also been extensively studied. Diuretics have been tried, especially in the first stage of CPT. However, they are not routinely used, because they can cause fluid and electrolyte imbalance and have only a marginal benefit in reducing peripheral edema. 51 , 52 Diuretics may also increase fibrosis because of worsening protein accumulation.
Benzopyrones are not routinely used in lymphedema treatment because of poor outcomes and varied formulations and dose regimens. 53 Once considered effective in the treatment of lymphedema by reducing edema fluid, softening limbs, and decreasing secondary infection, definitive conclusions about the efficacy of this medication are questionable with poor quality trials. 54 Liver toxicity is linked to high dosages of this drug; therefore they are not licensed for use in the United States, United Kingdom, Australia, or France. 55 Proponents claim that these drugs increase macrophage activity, encouraging the lysis of protein, which in turn reduces the formation of fibrotic tissue in the lymphedematous limb. 56 , 57
Antimicrobials have no role in reducing lymphedema and are intended to treat cellulitis, lymphangitis, or erysipelas. 40 To eradicate filaria from the bloodstream, diethylcarbamazine, albendazole, or ivermectin is recommended and may cause a variable inflammatory immune response by the host with aggravation of lymphatic blockage.
There is limited evidence from rigorously designed studies on the use of natural supplements for lymphedema. American horse chestnut has been reported to reduce venous edema but not lymphedema. 58 Selenium, a trace element nutrient that functions as a cofactor for a reduction of antioxidant enzymes, has been reported to improve lymphedema in head and neck cancer. 59 , 60 Bromelain, a substance found in pineapple, has antiinflammatory, anticoagulant, enzymatic, and diuretic effects. Some have wondered if bromelain use may be beneficial for lymphedema, but it has not been studied specifically for lymphedema but rather in malignancy and other diseases. 61 – 65
Because of the potential interactions with prescription drugs and other negative side effects, patients should check with their physician or health care provider before taking any natural supplement.
LASER THERAPY
Recent reports with small numbers of patients have demonstrated the efficacy of low-level laser therapy in reducing lymphedema, particularly after breast cancer. 66 – 69 A systematic review of 41 articles showed a reduction in limb volume in patients undergoing low-level laser therapy when compared with other treatments. However, because of a lack of comparison with complex physical therapy and other treatments, definitive conclusions about low-level laser therapy cannot be purported. 70 Additional studies with larger numbers of patients in diverse settings are needed to confirm these findings.
PNEUMOMASSAGE
IPC, also known as pneumomassage, is a two-phase program in which external gradient compression is applied by a pump, followed by elastic stockings or sleeves, to maintain edema reduction. IPC reduces edema by decreasing capillary filtration, and therefore lymph formation, rather than by accelerating lymph return. Single-chamber pumps, which were used in the past, are no longer used for lymphedema. Single-chamber pumps can cause fluid to move in both directions, even toward the edematous areas. Also, the pressure in single-chamber pumps does not stimulate lymphatic flow as sequential pumps do. 71 Acceptable pumps should have appliances (pump garments) with multiple chambers and sequential pressure delivery, with the chambers compressing in a specific pattern determined individually for the patient’s diagnosis and pattern of lymphedema. 72
Compliance is a concern with this approach, especially with the proximal displacement of edema and development of a fibrosclerotic ring at the root of the extremity or genitalia. Obstruction of lymph may occur, causing significant genital edema. The pumps may not be suitable for use in patients with coexisting renal failure or congestive heart failure. Patients whose lymphedema is the result of cancer treatment should ideally also be free of metastasis in the limb to prevent the risk of spreading the malignancy. 73 Studies of pneumomassage are conflicting; some illustrate immediate edema reduction and long-term success, whereas others show minimal improvement with use over time. 73 – 78 One study demonstrated considerable differences in skin or device interface pressure patterns and magnitude, which may have had an impact on therapeutic outcomes. 79 This is a significant concern because superficial structures may be harmed if the pressures applied in therapy are too high. 80 In general, lower pressures are considered safer, but the pressure must be individualized to the patient’s diagnosis and skin condition. IPC is not a “stand-alone” treatment.
EXERCISE AND ELEVATION
Exercise is a common rehabilitative intervention used to reduce lymphedema. Presently there is little evidence to indicate which types, intensities, and frequencies of exercise may be safely used in the management of lymphedema. However, specific exercise is beneficial for all patients. 81
Exercise improves muscular strength, cardiovascular function, psychological wellbeing, and functional capacity. Gentle resistance exercise stimulates muscle pumps and increases lymph flow; aerobic exercise increases intraabdominal pressure, which facilitates pumping of the thoracic duct. 82 , 83 Combinations of flexibility, resistance, and aerobic exercise may be beneficial in controlling lymphedema and should be tailored to the individual. 84 Patient-appropriate exercise enables the person with lymphedema to resume activity while minimizing the risk of exacerbation of swelling. 81 , 83 – 86 Physical therapy referral is required for patients who have difficulty with mobility, joint function, or joint movement.
Elevation of the affected limb, ideally to just above the level of the heart, is often advised to reduce swelling. Elevation acts by maximizing venous drainage and decreasing capillary pressure and lymph production.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


